

Prevalence and Survival Impact of Pretreatment Cancer-Associated Weight Loss: A Tool for Guiding Early Palliative Care
- PMID: 29466074
- PMCID: PMC5951294
- DOI: 10.1200/JOP.2017.025221
Prevalence and Survival Impact of Pretreatment Cancer-Associated Weight Loss: A Tool for Guiding Early Palliative Care
Abstract
Purpose: Cancer-associated weight loss is associated with poor prognosis in advanced malignancy; however, its pretreatment prevalence and survival impact are inadequately described in large cohorts. Such data, stratified by tumor type and stage, may facilitate the optimal and timely allocation of complementary care, leading to improvements in patient survival and quality of life.
Methods: We performed a retrospective cohort study of 3,180 consecutively treated adult patients with lung or GI (including colorectal, liver, and pancreatic) cancer. Pretreatment cancer-associated weight loss was based on the international consensus definition of cachexia. Prevalence and survival impact of pretreatment cancer-associated weight loss were evaluated using the Kaplan-Meier method and compared using log-rank test.
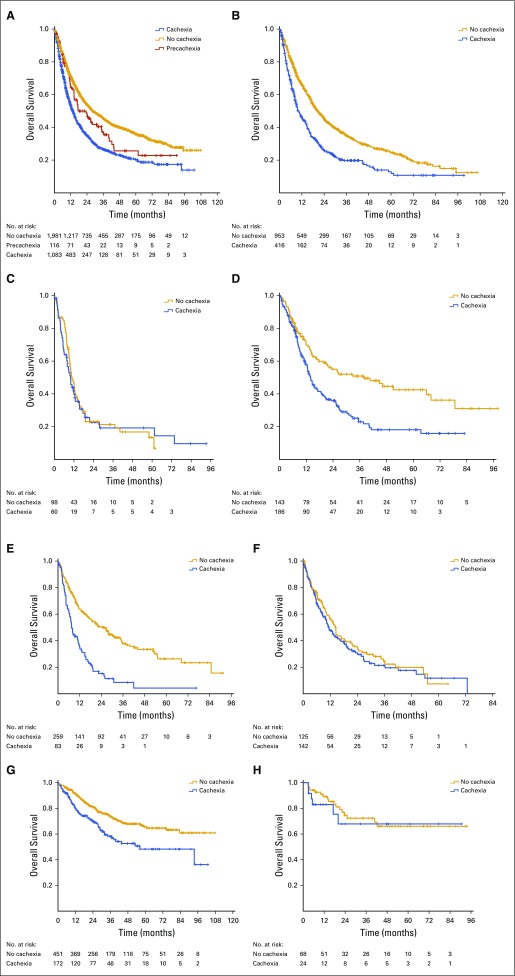
Results: Cancer-associated weight loss was observed at the time of cancer diagnosis in 34.1% of patients. Pretreatment weight loss was documented in 17.6%, 25.8%, 36.6%, and 43.3% of stage I, II, III, and IV cancers, respectively. Wasting was common regardless of tumor type, with prevalence at diagnosis ranging from 27.3% in patients with colorectal cancer to 53.4% in patients with gastroesophageal cancer. Pretreatment weight loss was associated with reduced overall survival after adjusting for stage, size, grade, comorbidity, age, sex, and tobacco history (hazard ratio, 1.26; 95% CI, 1.13 to 1.39).
Conclusion: Pretreatment cancer-associated weight loss is common, even in early-stage disease, and is independently associated with reduced survival. Minimal weight loss represents a clinically distinct entity with an associated overall survival intermediate to that of no weight loss and overt wasting. Early diagnosis and treatment of cancer-associated wasting offers a novel therapeutic avenue for reducing cancer mortality.
Figures
References
-
- Fearon K, Strasser F, Anker SD, et al. : Definition and classification of cancer cachexia: An international consensus. Lancet Oncol 12:489-495, 2011 - PubMed
-
- Blum D, Stene GB, Solheim TS, et al. : Validation of the consensus-definition for cancer cachexia and evaluation of a classification model: A study based on data from an international multicentre project (EPCRC-CSA). Ann Oncol 25:1635-1642, 2014 - PubMed
-
- Dewys WD, Begg C, Lavin PT, et al. : Prognostic effect of weight loss prior to chemotherapy in cancer patients. Am J Med 69:491-497, 1980 - PubMed
-
- Mariani L, Lo Vullo S, Bozzetti F: Weight loss in cancer patients: A plea for a better awareness of the issue. Support Care Cancer 20:301-309, 2012 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
