

Stroke survivors' and informal caregivers' experiences of primary care and community healthcare services - A systematic review and meta-ethnography
- PMID: 29466383
- PMCID: PMC5821463
- DOI: 10.1371/journal.pone.0192533
Stroke survivors' and informal caregivers' experiences of primary care and community healthcare services - A systematic review and meta-ethnography
Erratum in
-
Correction: Stroke survivors' and informal caregivers' experiences of primary care and community healthcare services - A systematic review and meta-ethnography.PLoS One. 2018 Apr 18;13(4):e0196185. doi: 10.1371/journal.pone.0196185. eCollection 2018. PLoS One. 2018. PMID: 29668761 Free PMC article.
Abstract
Objective: To describe and explain stroke survivors and informal caregivers' experiences of primary care and community healthcare services. To offer potential solutions for how negative experiences could be addressed by healthcare services.
Design: Systematic review and meta-ethnography.
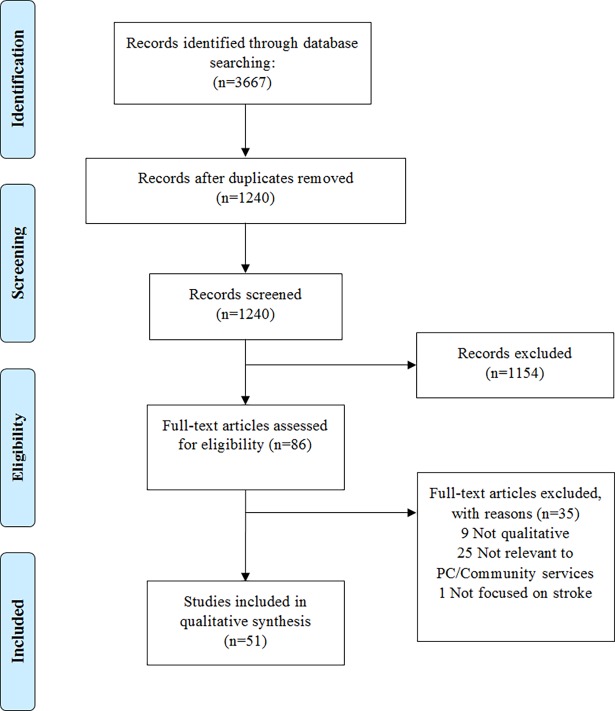
Data sources: Medline, CINAHL, Embase and PsycINFO databases (literature searched until May 2015, published studies ranged from 1996 to 2015).
Eligibility criteria: Primary qualitative studies focused on adult community-dwelling stroke survivors' and/or informal caregivers' experiences of primary care and/or community healthcare services.
Data synthesis: A set of common second order constructs (original authors' interpretations of participants' experiences) were identified across the studies and used to develop a novel integrative account of the data (third order constructs). Study quality was assessed using the Critical Appraisal Skills Programme checklist. Relevance was assessed using Dixon-Woods' criteria.
Results: 51 studies (including 168 stroke survivors and 328 caregivers) were synthesised. We developed three inter-dependent third order constructs: (1) marginalisation of stroke survivors and caregivers by healthcare services, (2) passivity versus proactivity in the relationship between health services and the patient/caregiver dyad, and (3) fluidity of stroke related needs for both patient and caregiver. Issues of continuity of care, limitations in access to services and inadequate information provision drove perceptions of marginalisation and passivity of services for both patients and caregivers. Fluidity was apparent through changing information needs and psychological adaptation to living with long-term consequences of stroke.
Limitations: Potential limitations of qualitative research such as limited generalisability and inability to provide firm answers are offset by the consistency of the findings across a range of countries and healthcare systems.
Conclusions: Stroke survivors and caregivers feel abandoned because they have become marginalised by services and they do not have the knowledge or skills to re-engage. This can be addressed by: (1) increasing stroke specific health literacy by targeted and timely information provision, and (2) improving continuity of care between specialist and generalist services.
Systematic review registration number: PROSPERO 2015:CRD42015026602.
Conflict of interest statement
Figures


References
-
- Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, Bennett DA, et al. Global and regional burden of stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet. 2014;383(9913):245–54. doi: 10.1016/S0140-6736(13)61953-4 ; PubMed Central PMCID: 24449944. - DOI - PMC - PubMed
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–128. doi: 10.1016/S0140-6736(12)61728-0 ; PubMed Central PMCID: 23245604. - DOI - PMC - PubMed
-
- Saka Ö, McGuire A, Wolfe C. Cost of stroke in the United Kingdom. Age Ageing. 2009;38(1):27–32. doi: 10.1093/ageing/afn281 ; PubMed Central PMCID: 19141506. - DOI - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics-2016 Update: a report from the American Heart Association. Circulation. 2016;133(4):e38–360. Epub 2015/12/18. doi: 10.1161/CIR.0000000000000350 ; PubMed Central PMCID: 26673558. - DOI - PubMed
-
- Deloitte Access Economics. The economic impact of stroke in Australia Deloitte Access Economics, 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
