

Performance of loop-mediated isothermal amplification assay in the diagnosis of pulmonary tuberculosis in a high prevalence TB/HIV rural setting in Uganda
- PMID: 29466946
- PMCID: PMC5822669
- DOI: 10.1186/s12879-018-2992-1
Performance of loop-mediated isothermal amplification assay in the diagnosis of pulmonary tuberculosis in a high prevalence TB/HIV rural setting in Uganda
Abstract
Background: Smear microscopy lacks sensitivity especially in HIV co-infection, resulting in undiagnosed tuberculosis (TB) and high mortality. The loop-mediated isothermal amplification (TB-LAMP) assay can be staged with minimal infrastructure, is rapid, low cost and detection can be with the naked eye. We assessed feasibility and performance of Eiken TB-LAMP test at point-of-need in TB diagnosis in a high prevalence TB/HIV rural setting in Uganda.
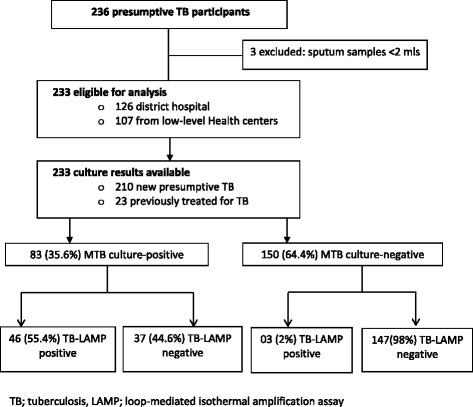
Methods: From October 2013-February 2014, TB-LAMP testing was performed on sputum specimens from outpatient presumptive TB adults at a district hospital and two low-level health centers in Kiboga District where smear microscopy is the available routine diagnostic option. TB-LAMP was performed by a technician after a week of training in the district hospital. The technician had no prior experience in the technology. Samples from the low-level health centers were transported to the district hospital for TB-LAMP.
Results: Of the 233 presumptive TB (126 at hospital); 113 (48.5%) were HIV-infected; 129 (55%) male; median age 40 (IQR 30-53). Compared to MTB culture, overall sensitivity and specificity of TB-LAMP were 55.4% (95 CI 44.1-66.3) and 98.0% (95 CI 94.3-99.6) respectively. Among HIV-infected participants, TB-LAMP sensitivity and specificity were 52.3% (95 CI 36.7-67.5%) and 97.1% (95 CI 89.9-99.6) respectively; and 24.4% (95% CI 12.9-39.5) and 98.6% (95% CI 95.1-99.8) respectively among smear-negatives. TB-LAMP sensitivity and specificity were 62.2% (95% CI 44.8-77.5) and 97.8% (95% CI 92.1-99.7) in the hospital setting where central testing occurred compared to 50.0% (95% CI 34.9-65.1) and 98.4% (95% CI 91.2-100) respectively in low-level health centers where specimens were transported centrally.
Conclusions: In this high prevalence TB/HIV rural setting, TB-LAMP performs better than conventional smear microscopy in diagnosis of MTB among presumptive TB patients although the sensitivity is lower than that reported by the World Health Organization. TB-LAMP can easily be performed following a short training period and in absence of sophisticated infrastructure and expertise.
Keywords: Diagnostic; LAMP; Microscopy; Rural; Tuberculosis; Uganda.
Conflict of interest statement
Ethics approval and consent to participate
Approval for this study was granted by the Scientific Review Board of the Infectious Diseases Institute (IDI), the Institutional Review Boards of the Joint Clinical Research Centre, Kampala, Uganda and the Uganda National Council for Science and Technology (Ref # HS 1486). A waiver of informed consent was granted by the Scientific Review Board of the Infectious Diseases Institute (IDI), the Institutional Review Boards of the Joint Clinical Research Centre, Kampala, Uganda and the Uganda National Council for Science and Technology. Waiver of consent was allowed since no unique personal identifying information was collected by the study team and there was no direct interaction with patients. Waiver of informed consent did not adversely affect the rights and welfare of individuals whose specimens were used. The results of all testing were made available to clinicians for clinical care.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
-
- WHO: World Health Organization. Global tuberculosis report. 2016. http://apps.who.int/medicinedocs/documents/s23098en/s23098en.pdf. Downloaded on May 13, 2017.
-
- Colebunders R, Bastian I. A review of the diagnosis and treatment of smear-negative pulmonary tuberculosis. Int J Tuberc Lung Dis. 2000;4(2):97–107. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
