

The benefits of co-location in primary care practices: the perspectives of general practitioners and patients in 34 countries
- PMID: 29466980
- PMCID: PMC5822600
- DOI: 10.1186/s12913-018-2913-4
The benefits of co-location in primary care practices: the perspectives of general practitioners and patients in 34 countries
Abstract
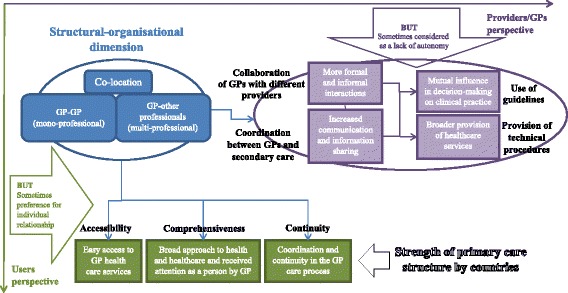
Background: There is no clear evidence as to whether the co-location of primary care professionals in the same facility positively influences their way of working and the quality of healthcare as perceived by patients. The aim of this study was to identify the relationships between general practitioner (GP) co-location with other GPs and/or other professionals and the GP outcomes and patients' experiences.
Methods: We wanted to test whether GP co-location is related to a broader range of services provided, the use of clinical governance tools and inter-professional collaboration, and whether the patients of co-located GPs perceive a better quality of care in terms of accessibility, comprehensiveness and continuity of care with their GPs. The source of data was the QUALICOPC study (Quality and Costs of Primary Care in Europe), which involved surveys of GPs and their patients in 34 countries, mostly in Europe. In order to study the relationships between GP co-location and both GPs' outcomes and patients' experience, multilevel linear regression analysis was carried out.
Results: The GP questionnaire was filled in by 7183 GPs and the patient experience questionnaire by 61,931 patients. Being co-located with at least one other professional is the most common situation of the GPs involved in the study. Compared with single-handed GP practices, GP co-location are positively associated with the GP outcomes. Considering the patients' perspective, comprehensiveness of care has the strongest negative relationship of GP co-location of all the dimensions of patient experiences analysed.
Conclusions: The paper highlights that GP mono- and multi-disciplinary co-location is related to positive outcomes at a GP level, such as a broader provision of technical procedures, increased collaboration among different providers and wider coordination with secondary care. However, GP co-location, particularly in a multidisciplinary setting, is related to less positive patient experiences, especially in countries with health systems characterised by a weak primary care structure.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was acquired in accordance with the legal requirements in each country. Depending on the national requirements, written or oral informed consent was requested [21].
In the following table we report an overview of the ethics committees in each country.
aSee: Wong ST, Chau LW, Hogg W et al. An international cross-sectional survey on the Quality and Costs of Primary Care (QUALICO-PC): recruitment and data collection of places delivering primary care across Canada. BMC Family Practice (2015) 16:20.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Afrite A, Bourgueil Y, Daniel F, Mousquèsa F, Couralet PE, Chevillard G. The impact of multi-professional group practices on healthcare supply. Evaluation aims and methods for “maisons”, “pôles de santé” and “centres de santé” within the framework of experiments with new mechanisms of remuneration. Questions d’économie de la santé. 2013;189:1–6.
-
- Blount A. Integrated primary care: organizing the evidence. Families,Systems Health. 2003;21(2):121–123. doi: 10.1037/1091-7527.21.2.121. - DOI
-
- Bonciani M, Barsanti S, Matarrese D. Esperienze di integrazione nell’assistenza primaria basate sulla co-location dei servizi: quali prospettive per il modello della Casa della Salute? Mecosan. 2015;96:81–122.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
