

Editorial
doi: 10.1186/s13054-018-1970-8.
What is new in critical care echocardiography?
Affiliations
- PMID: 29467026
- PMCID: PMC5822525
- DOI: 10.1186/s13054-018-1970-8
Item in Clipboard
Editorial
What is new in critical care echocardiography?
Crit Care.
.
No abstract available
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The author declares that he has no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
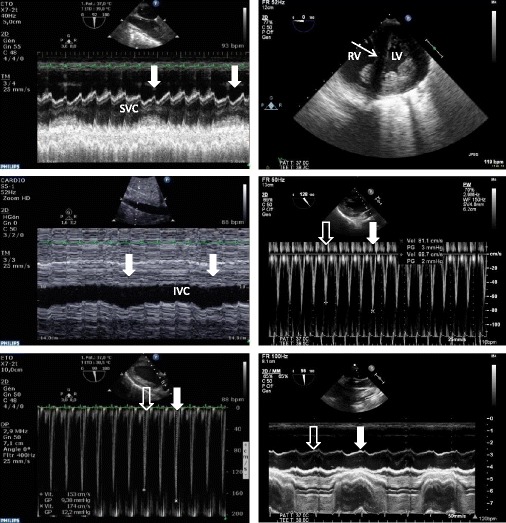
Hemodynamic assessment using transesophageal echocardiography in two patients presenting with shock of distinct origin. In the first patient (left panels), inadequate cardiac output was ascribed to a persisting preload dependence, as reflected by concordant and significant respiratory variations (closed thick white arrow: mechanical insufflation) of the superior vena cava (SVC) diameter (upper left, collapsibility index), of the inferior vena cava (IVC; middle left, distensibility index), and of maximal Doppler velocity recorded in the left ventricular outflow tract (lower left, open thick arrow: expiration phase). In this patient, cardiac output significantly increased after fluid loading. In the second patient who was under protective mechanical ventilation for an acute respiratory distress syndrome (right panels) and exhibited tissue hypoperfusion, a 15% pulse pressure variation suggested fluid responsiveness. Transesophageal echocardiography disclosed an enlarged right ventricle (RV) in conjunction with a paradoxical septal motion consistent with an acute cor pulmonale (upper right, thin arrow) and significant respiratory variations of maximal Doppler velocity recorded in the left ventricular outflow tract (middle right, open thick arrow: expiration phase; closed thick arrow: mechanical insufflation). Nevertheless, the absence of any respiratory variations of the superior vena cava diameter suggested the absence of fluid responsiveness, but rather a systemic venous congestion associated with acute cor pulmonale (lower right). Accordingly, both pulse pressure variation and respiratory variations of maximal Doppler velocity recorded in the left ventricular outflow tract were interpreted as false-positive results. Blood volume expansion was considered potentially inefficient and detrimental, ventilator settings were modified, and inhaled nitric oxide was initiated to further unload the right ventricle. LV left ventricle
References
-
- Prat G, Charron C, Repesse X, Coriat P, Bailly P, L'her E, Vieillard-Baron A. The use of computerized echocardiographic simulation improves the learning curve for transesophageal hemodynamic assessment in critically ill patients. Ann Intensive Care. 2016;6:27. doi: 10.1186/s13613-016-0132-x. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
