

A pilot study of a Medication Rationalization (MERA) intervention
- PMID: 29467186
- PMCID: PMC5878954
- DOI: 10.9778/cmajo.20170134
A pilot study of a Medication Rationalization (MERA) intervention
Abstract
Background: Many seriously ill and frail inpatients receive potentially inappropriate or harmful medications and do not receive medications for symptoms of advanced illness. We developed and piloted an interprofessional Medication Rationalization (MERA) approach to deprescribing inappropriate medications and prescribing appropriate comfort medications.
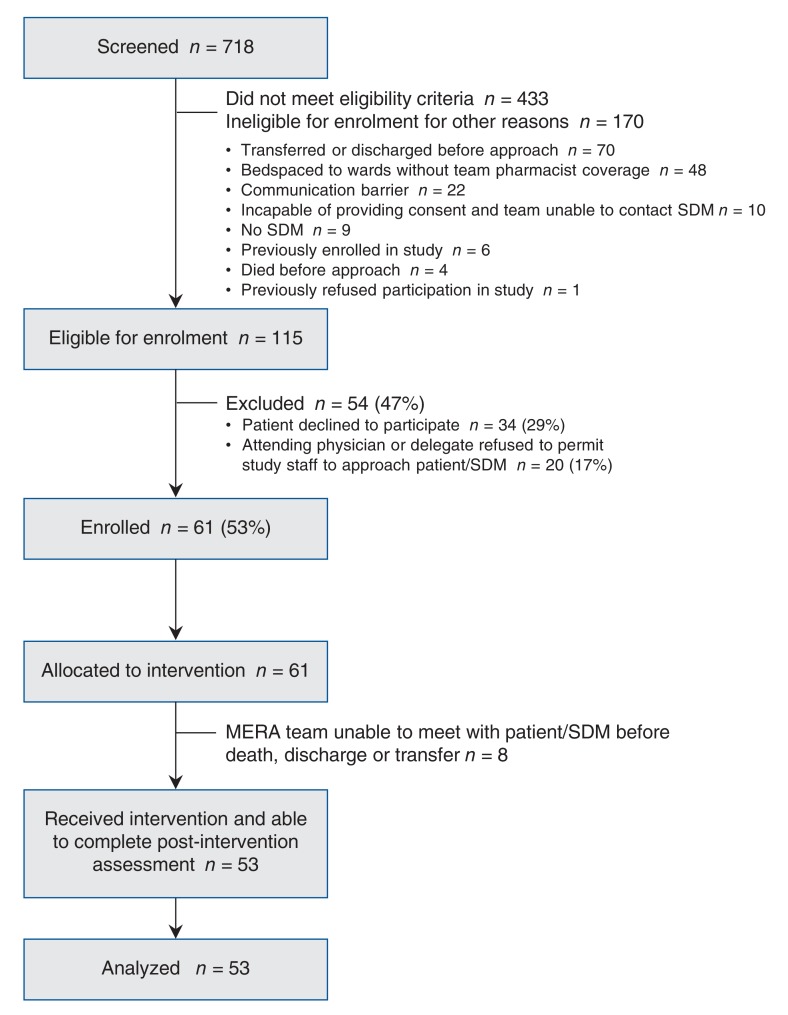
Methods: We conducted a single-centre pilot study of inpatients at risk of 6-month mortality from advanced age or morbidity. The MERA team reviewed the patients' medications and made recommendations on the basis of guidelines. We measured end points for feasibility, acceptability, efficiency and effectiveness.
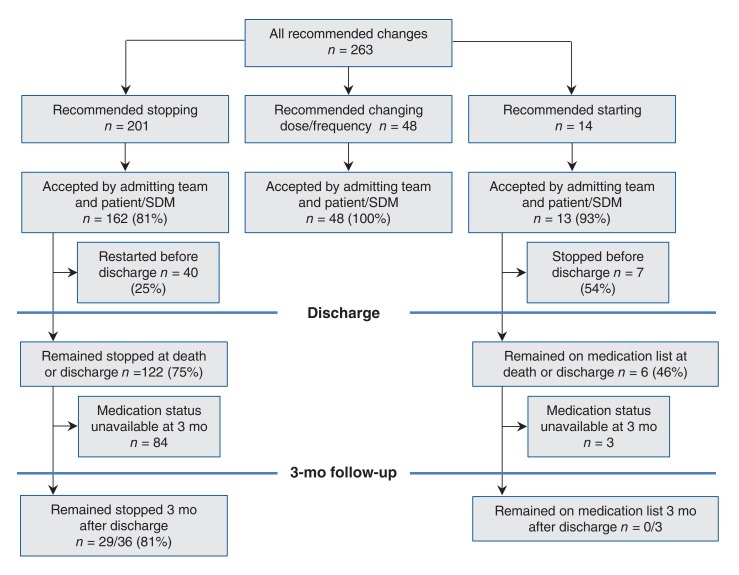
Results: We enrolled 61 of 115 (53%) eligible patients with a mean age of 79.6 years (standard deviation [SD] 11.7 yr). Patients were taking an average of 11.5 (SD 5.2) medications before admission and had an average of 2.1 symptoms with greater than 6/10 severity on the revised Edmonton Symptom Assessment System. The MERA team recommended 263 medication changes, of which 223 (85%) were accepted by both the medical team and the patient. MERA team's recommendations resulted in the discontinuation of 162 medications (mean 3.1 per patient), dose changes for 48 medications (mean 0.9 per patient) and the addition of 13 medications (mean 0.2 per patient). Patients who received the MERA intervention stopped significantly more inappropriate medications than similar non-MERA comparison patients for whom data were collected retrospectively (3.1 v. 0.9 medications per patient, p < 0.01). The MERA approach was highly acceptable to patients and medical team members.
Interpretation: The MERA intervention is feasible, acceptable, efficient and possibly effective for changing medication use among seriously ill and frail elderly inpatients. Scalability and effectiveness may be improved through automation and integration with medication reconciliation programs.
Copyright 2018, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: James Downar has received a grant from Boehringer Ingelheim (Canada) and personal fees from Boehringer Ingelheim (Canada), Medtronic and Novartis for reasons unrelated to this study. No other competing interests were declared.
Figures
References
-
- Ma G, Downar J. Noncomfort medication use in acute care inpatients comanaged by palliative care specialists near the end of life: a cohort study. Am J Hosp Palliat Care. 2013;31:812–9. - PubMed
-
- Downar J, Rodin D, Barua R, et al. Rapid response teams, do not resuscitate orders, and potential opportunities to improve end-of-life care: a multicentre retrospective study. J Crit Care. 2013;28:498–503. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources