

Evaluation of a Portable Doppler Ultrasound Gating Device for Fetal Cardiac MR Imaging: Initial Results at 1.5T and 3T
- PMID: 29467359
- PMCID: PMC6196307
- DOI: 10.2463/mrms.mp.2017-0100
Evaluation of a Portable Doppler Ultrasound Gating Device for Fetal Cardiac MR Imaging: Initial Results at 1.5T and 3T
Abstract
Purpose: Fetal cardiac MRI has the potential to play an important role in the assessment of fetal cardiac pathologies, but it is up to now not feasible due to a missing gating method. The purpose of this work was the evaluation of Doppler ultrasound (DUS) for external fetal cardiac gating with regard to compatibility, functionality, and reliability. Preliminary results were assessed performing fetal cardiac MRI.
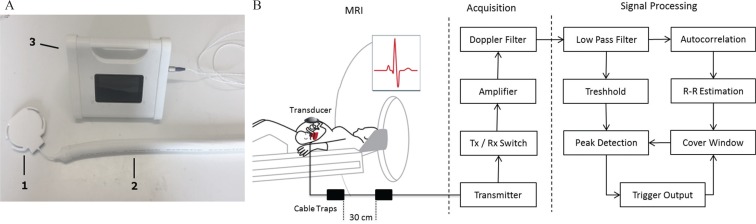
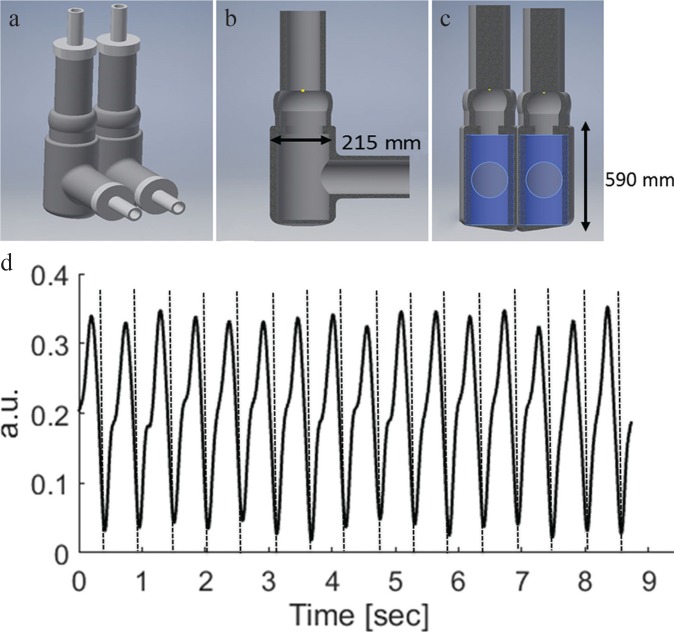
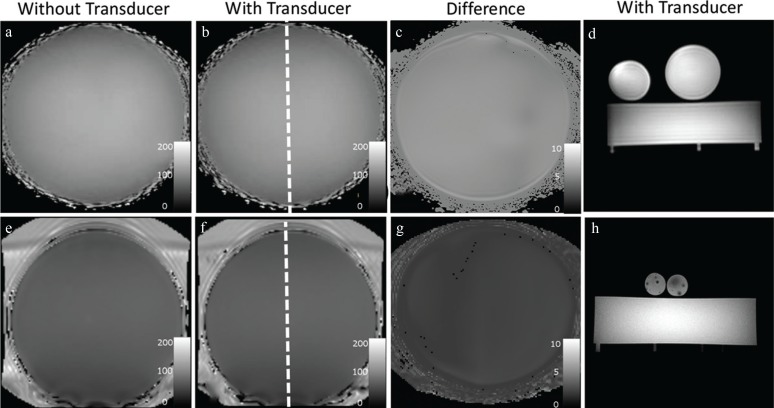
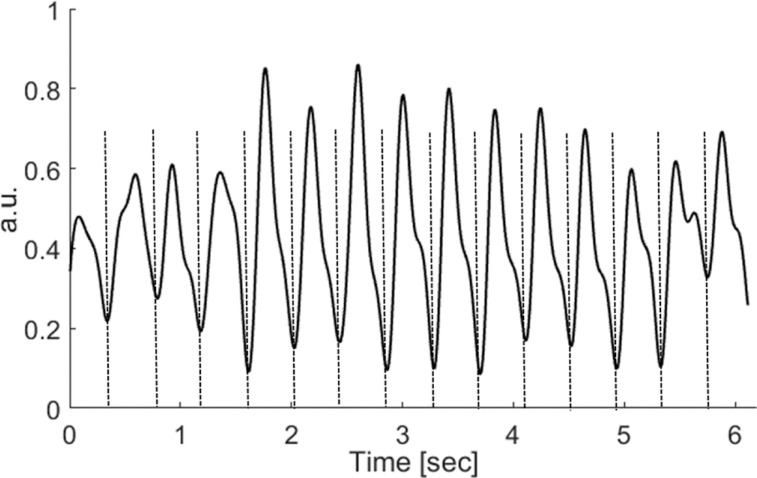
Methods: An MRI conditional DUS device was developed to obtain a gating signal from the fetal heart. The MRI compatibility was evaluated at 1.5T and 3T using B1 field maps and gradient echo images. The quality and sensitivity of the DUS device to detect the fetal heart motion for cardiac gating were evaluated outside the MRI room in 15 fetuses. A dynamic fetal cardiac phantom was employed to evaluate distortions of the DUS device and gating signal due to electromagnetic interferences at 1.5T and 3T. In the first in vivo experience, dynamic fetal cardiac images were acquired in four-chamber view at 1.5T and 3T in two fetuses.
Results: The maximum change in the B1 field and signal intensity with and without the DUS device was <6.5% for 1.5T and 3T. The sensitivity of the DUS device to detect the fetal heartbeat was 99.1%. Validation of the DUS device using the fetal cardiac phantom revealed no electromagnetic interferences at 1.5T or 3T and a high correlation to the simulated heart frequencies. Fetal cardiac cine images were successfully applied and showed good image quality.
Conclusion: An MR conditional DUS gating device was developed and evaluated revealing safety, compatibility, and reliability for different field strengths. In a preliminary experience, the DUS device was successfully applied for in vivo fetal cardiac imaging at 1.5T and 3T.
Keywords: Doppler ultrasound; cardiovascular system; fetal heart; magnetic resonance imaging.
Conflict of interest statement
The authors C. Ruprecht, K. Fehrs, and F. Kording are inventor and shareholder of the pending patent WO 2017/102924 A1 “Ultrasonic Device for Detecting the Heartbeat of a Patient”. No money has been paid to any of the authors or the related institutions.
Figures



References
-
- Allan L. Technique of fetal echocardiography. Pediatr Cardiol 2004; 25:223–233. - PubMed
-
- Hunter LE, Simpson JM. Prenatal screening for structural congenital heart disease. Nat Rev Cardiol 2014; 11:323–334. - PubMed
-
- Wielandner A, Mlczoch E, Prayer D, Berger-Kulemann V. Potential of magnetic resonance for imaging the fetal heart. Semin Fetal Neonatal Med 2013; 18:286–297. - PubMed
-
- Forbus GA, Atz AM, Shirali GS. Implications and limitations of an abnormal fetal echocardiogram. Am J Cardiol 2004; 94:688–689. - PubMed
-
- Levi S. Ultrasound in prenatal diagnosis: polemics around routine ultrasound screening for second trimester fetal malformations. Prenat Diagn 2002; 22:285–295. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical