

Utility of SOFA score, management and outcomes of sepsis in Southeast Asia: a multinational multicenter prospective observational study
- PMID: 29468069
- PMCID: PMC5813360
- DOI: 10.1186/s40560-018-0279-7
Utility of SOFA score, management and outcomes of sepsis in Southeast Asia: a multinational multicenter prospective observational study
Abstract
Background: Sepsis is a global threat but insufficiently studied in Southeast Asia. The objective was to evaluate management, outcomes, adherence to sepsis bundles, and mortality prediction of maximum Sequential Organ Failure Assessment (SOFA) scores in patients with community-acquired sepsis in Southeast Asia.
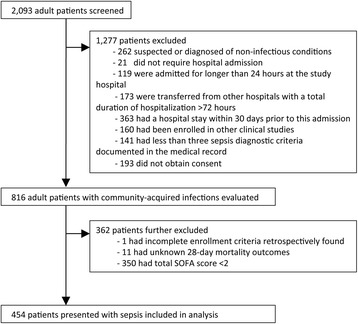
Methods: We prospectively recruited hospitalized adults within 24 h of admission with community-acquired infection at nine public hospitals in Indonesia (n = 3), Thailand (n = 3), and Vietnam (n = 3). In patients with organ dysfunction (total SOFA score ≥ 2), we analyzed sepsis management and outcomes and evaluated mortality prediction of the SOFA scores. Organ failure was defined as the maximum SOFA score ≥ 3 for an individual organ system.
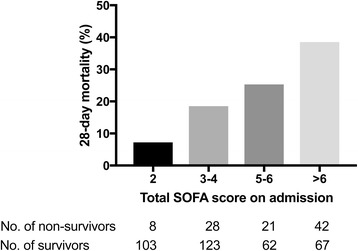
Results: From December 2013 to December 2015, 454 adult patients presenting with community-acquired sepsis due to diverse etiologies were enrolled. Compliance with sepsis bundles within 24 h of admission was low: broad-spectrum antibiotics in 76% (344/454), ≥ 1500 mL fluid in 50% of patients with hypotension or lactate ≥ 4 mmol/L (115/231), and adrenergic agents in 71% of patients with hypotension (135/191). Three hundred and fifty-five patients (78%) were managed outside of ICUs. Ninety-nine patients (22%) died. Total SOFA score on admission of those who subsequently died was significantly higher than that of those who survived (6.7 vs. 4.6, p < 0.001). The number of organ failures showed a significant correlation with 28-day mortality, which ranged from 7% in patients without any organ failure to 47% in those with failure of at least four organs (p < 0.001). The area under the receiver operating characteristic curve of the total SOFA score for discrimination of mortality was 0.68 (95% CI 0.62-0.74).
Conclusions: Community-acquired sepsis in Southeast Asia due to a variety of pathogens is usually managed outside the ICU and with poor compliance to sepsis bundles. In this population, calculation of SOFA scores is feasible and SOFA scores are associated with mortality.
Trial registration: ClinicalTrials.gov, NCT02157259. Registered 5 June 2014, retrospectively registered.
Keywords: Asia, Southeastern; Organ dysfunction scores; Patient care bundles; Sepsis.
Conflict of interest statement
The study protocol (NCT02157259) and related documents were approved by regional and national Ethics Committees. Consent was provided by participants or representatives of participants as appropriate before participating.Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
