

Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis
- PMID: 29468365
- PMCID: PMC5895684
- DOI: 10.1007/s00247-018-4093-0
Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis
Abstract
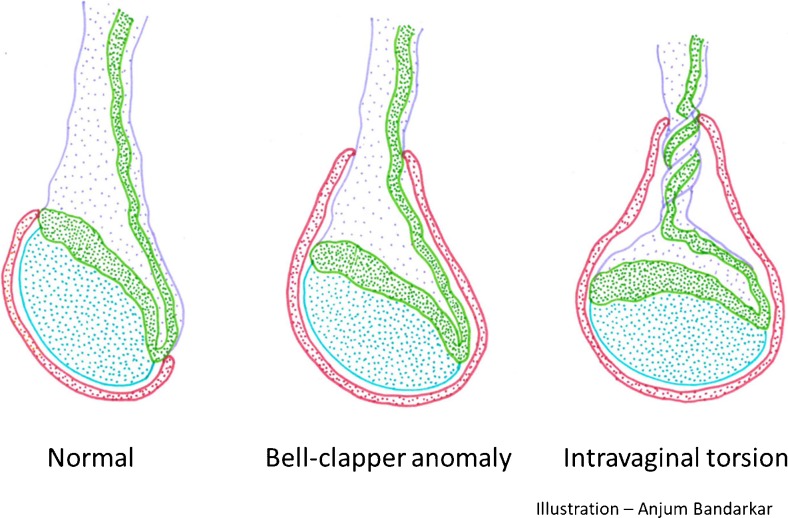
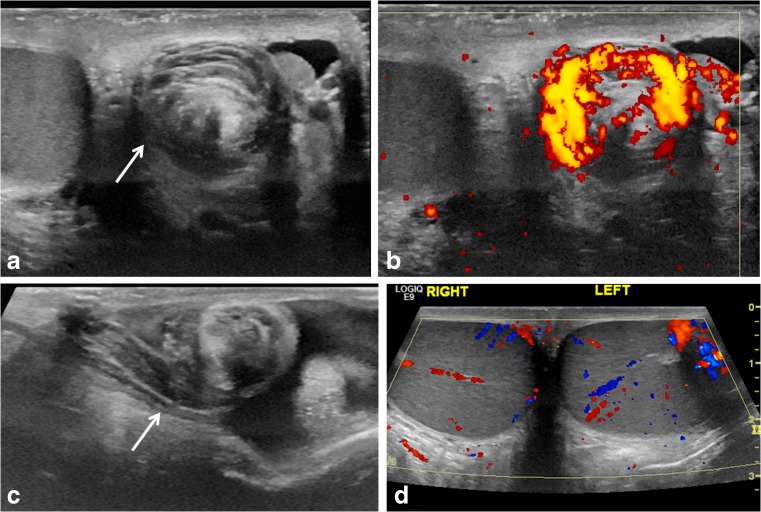
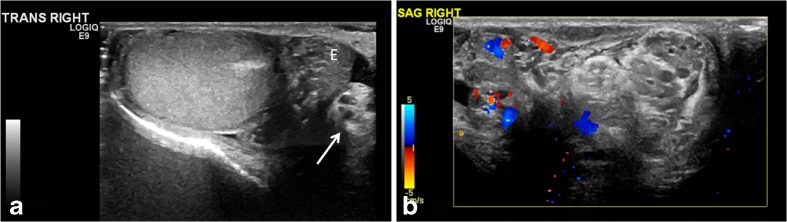
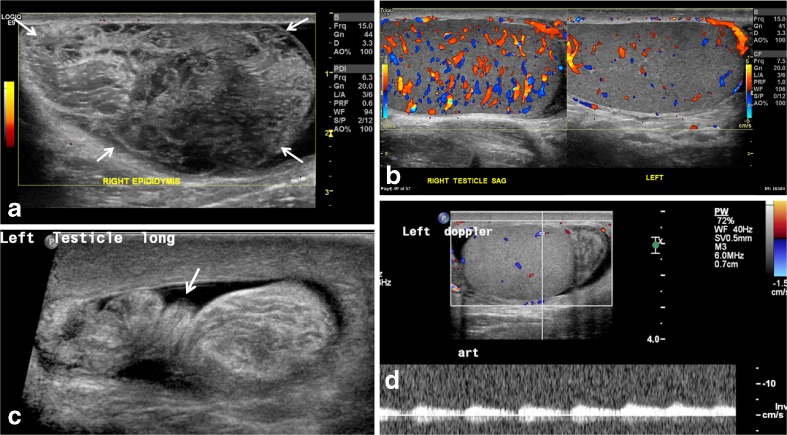
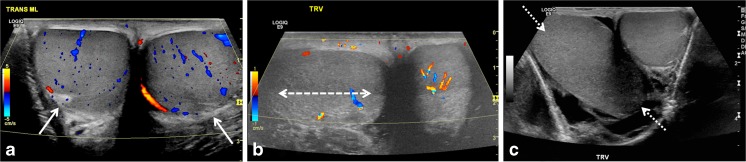
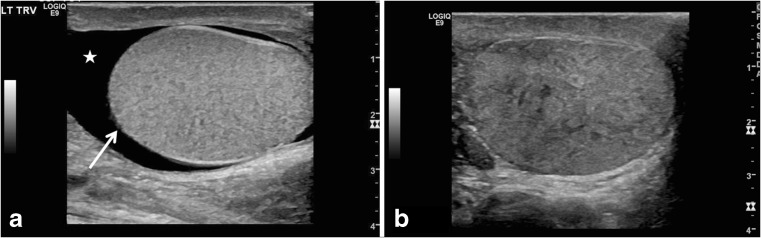
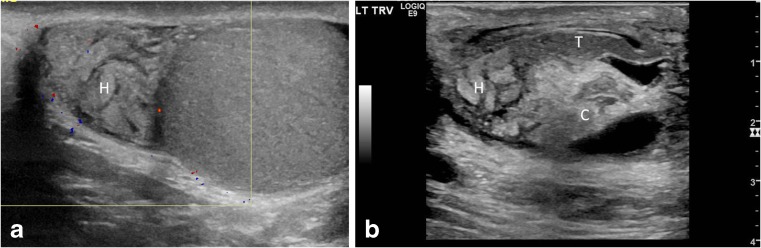
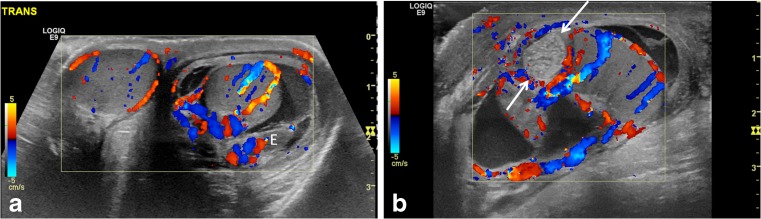
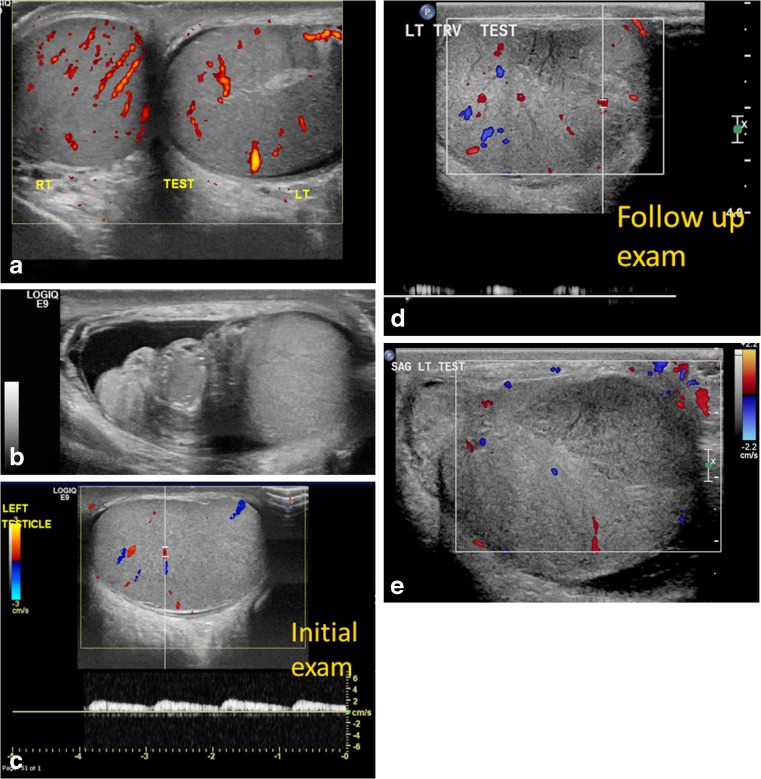
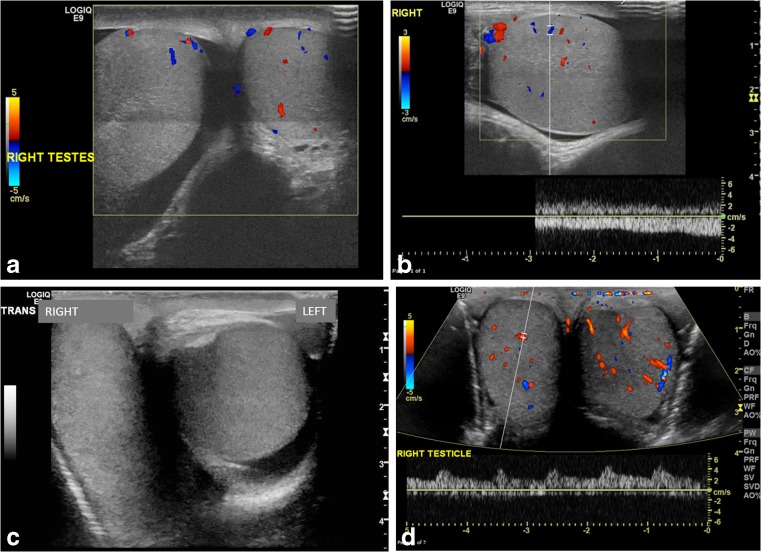
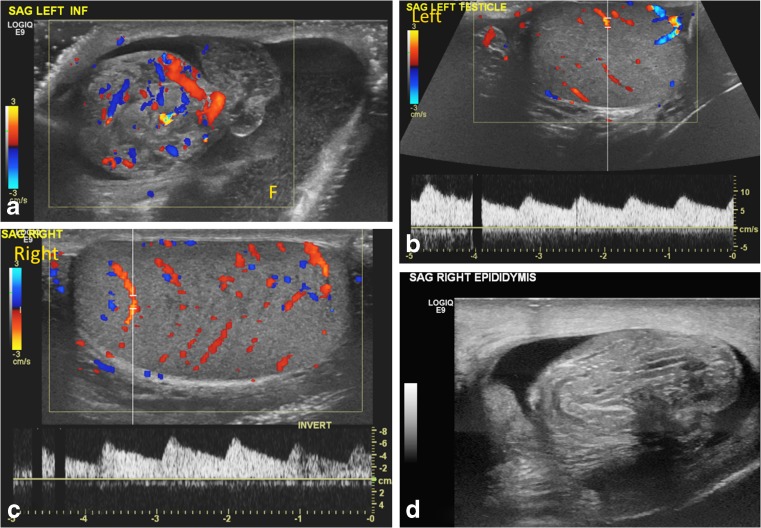
Testicular sonography has contributed greatly to the preoperative diagnosis of testicular torsion in the pediatric patient and is the mainstay for evaluation of acute scrotal pain. Despite its high sensitivity and specificity, both false-negative and false-positive findings occur. Presence of documented Doppler flow within the testis might be a dissuading factor for surgical exploration with resultant testicular loss in the false-negative cases. Our goal is to illustrate key sonographic features in the spectrum of testicular torsion with preserved testicular flow, and to describe how to differentiate testicular torsion from epididymitis in order to avoid the under-diagnosis of testicular torsion. We simplify the anatomy of the bell clapper testis. We also describe our sonographic protocol for testicular torsion and share valuable tips from our approach to challenging cases.
Keywords: Bell clapper anomaly; Children; Epididymis; Scrotum; Testis; Torsion; Ultrasound; Whirlpool sign.
Conflict of interest statement
None
Figures
References
-
- Vikram S, Bhatt S, Rubens D. Sonographic evaluation of testicular torsion. Ultrasound Clinics. 2006;1:55–66. doi: 10.1016/j.cult.2005.09.006. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
