

15 Years of Experience with Biphasic Insulin Aspart 30 in Type 2 Diabetes
- PMID: 29468559
- PMCID: PMC5833912
- DOI: 10.1007/s40268-018-0228-x
15 Years of Experience with Biphasic Insulin Aspart 30 in Type 2 Diabetes
Abstract
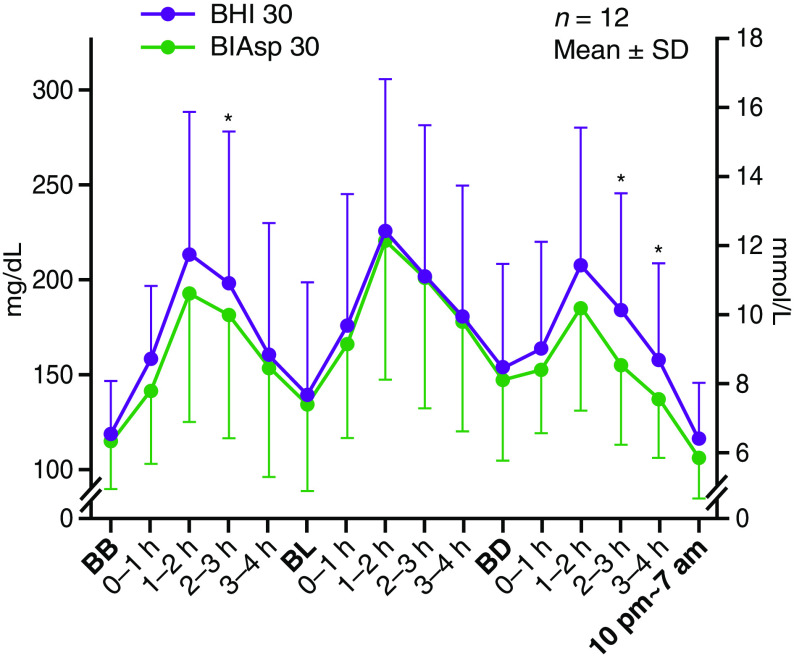
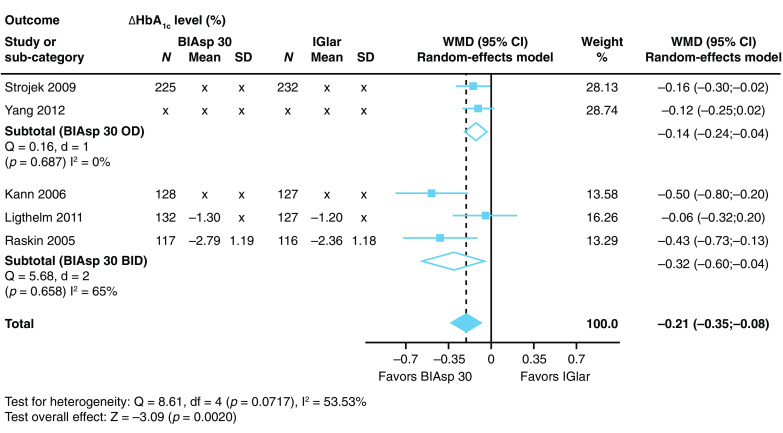
Since clinical experience with biphasic insulin aspart 30 (BIAsp 30) in type 2 diabetes mellitus (T2DM) was reviewed in 2012 after 10 years of use worldwide, additional studies have been published that highlight new aspects, including use in real-world populations. Evidence from 35 new studies confirms and builds upon previous work indicating that BIAsp 30 continues to have pharmacodynamic and clinical advantages over biphasic human insulin (BHI 30), including in real-world practice with unselected populations of patients. BIAsp 30 has also been shown to be safe and efficacious as an add-on to dipeptidyl peptidase-4 (DPP-4) inhibitors. Intensification with BIAsp 30 is a safe and effective way to improve glycemic control, and titration performed by patients can achieve results that are at least comparable to those when being guided by healthcare providers. Stepwise intensification using BIAsp 30 is comparable to intensification using a basal-bolus regimen, and twice-daily BIAsp 30 provides similar glycemic control to a basal-plus regimen. Data from large observational studies, in particular, have identified patient-related characteristics that are associated with improved clinical responses, suggesting that earlier initiation and intensification of therapy is warranted. Finally, new health-economic analyses continue to confirm that BIAsp 30 is cost effective versus other therapies such as BHI 30, neutral protamine Hagedorn (NPH), or insulin glargine in both insulin-naïve and insulin-experienced patients. After 15 years of clinical use worldwide, analysis of more recent 5-year data indicates that BIAsp 30 remains a safe, effective, and simple-to-use insulin for initiation and intensification by diabetes specialists and primary care physicians in a variety of patients with T2DM.
Conflict of interest statement
AL has received funding for membership on Novo Nordisk and Eli Lilly advisory boards and/or consulting services and for lectures from Novo Nordisk, Eli Lilly, Sanofi, Boehringer-Ingelheim, AstraZeneca, Roche, and MSD. VM has received research grants and honoraria from Novo Nordisk, Sanofi, MSD, Johnson & Johnson, and Eli Lilly and lecture fees from Novo Nordisk. WY has attended advisory boards and been a speaker for Novo Nordisk. KS has received honoraria for speaking engagements from Eli Lilly, Novo Nordisk, Sanofi-Aventis, Servier, Boehringer-Ingelheim, and Polfa-Tarchomin and has participated in clinical trials for AstraZeneca, Pfizer, and Amgen. SL has received funding for advisory activities from Novo Nordisk and for speaker activities from Novo Nordisk, Novartis Pharma AG, Roche Pharmaceuticals, and AstraZeneca Pharmaceuticals LP.
Figures
References
-
- Rys P, Wojciechowski P, Siejka S, Małecki P, Hak L, Malecki MT. A comparison of biphasic insulin aspart and insulin glargine administered with oral antidiabetic drugs in type 2 diabetes mellitus–a systematic review and meta-analysis. Int J Clin Pract. 2014;68:304–313. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
