

A Magnetic Resonance Imaging-Based Prediction Model for Prostate Biopsy Risk Stratification
- PMID: 29470570
- PMCID: PMC5885194
- DOI: 10.1001/jamaoncol.2017.5667
A Magnetic Resonance Imaging-Based Prediction Model for Prostate Biopsy Risk Stratification
Abstract
Importance: Multiparametric magnetic resonance imaging (MRI) in conjunction with MRI-transrectal ultrasound (TRUS) fusion-guided biopsies have improved the detection of prostate cancer. It is unclear whether MRI itself adds additional value to multivariable prediction models based on clinical parameters.
Objective: To determine whether an MRI-based prediction model can reduce unnecessary biopsies in patients with suspected prostate cancer.
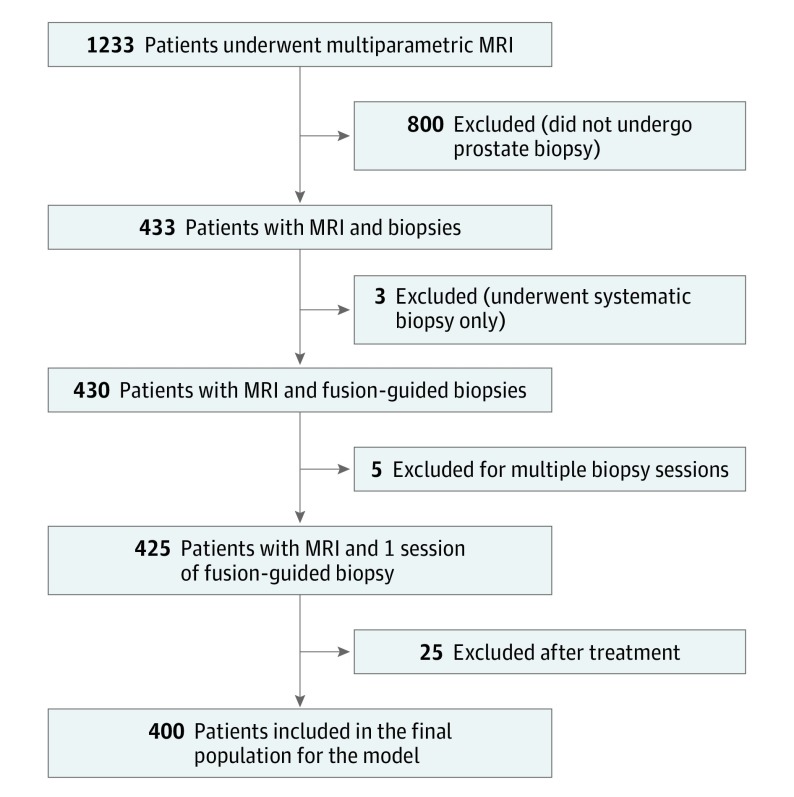
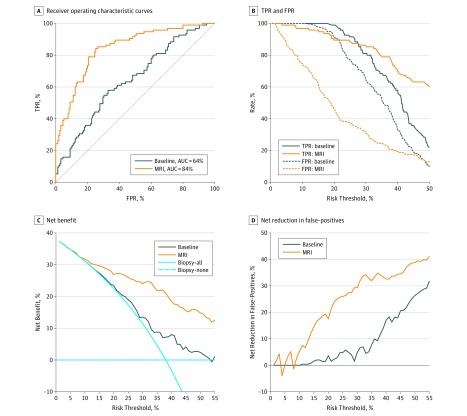
Design, setting, and participants: Patients underwent MRI, MRI-TRUS fusion-guided biopsy, and 12-core systematic biopsy in 1 session. The development cohort used to derive the prediction model consisted of 400 patients from 1 institution enrolled between May 14, 2015, and August 31, 2016, and the validation cohort included 251 patients from 2 independent institutions who underwent biopsies between April 1, 2013, and June 30, 2016, at 1 institution and between July 1, 2015, and October 31, 2016, at the other institution. The MRI model included MRI-derived parameters in addition to clinical variables. Area under the curve of receiver operating characteristic curves and decision curve analysis were performed.
Main outcomes and measures: Risk of clinically significant prostate cancer on biopsy, defined as a Gleason score of 3 + 4 or higher in at least 1 biopsy core.
Results: Overall, 193 (48.3%) of the 400 patients in the development cohort (mean [SD] age at biopsy, 64.3 [7.1] years) and 96 (38.2%) of the 251 patients in the validation cohort (mean [SD] age at biopsy, 64.9 [7.2] years) had clinically significant prostate cancer, defined as a Gleason score greater than or equal to 3 + 4. By applying the model to the external validation cohort, the area under the curve increased from 64% to 84% compared with the baseline model (P < .001). At a risk threshold of 20%, the MRI model had a lower false-positive rate than the baseline model (46% [95% CI, 32%-66%] vs 92% [95% CI, 70%-100%]), with only a small reduction in the true-positive rate (89% [95% CI, 85%-96%] vs 99% [95% CI, 89%-100%]). Eighteen of 100 fewer biopsies could have been performed, with no increase in the number of patients with missed clinically significant prostate cancers.
Conclusions and relevance: The inclusion of MRI-derived parameters in a risk model could reduce the number of unnecessary biopsies while maintaining a high rate of diagnosis of clinically significant prostate cancers.
Conflict of interest statement
Figures
Comment in
-
Magnetic Resonance Imaging-Based Prediction of Prostate Cancer Risk.JAMA Oncol. 2018 Nov 1;4(11):1624-1625. doi: 10.1001/jamaoncol.2018.4221. JAMA Oncol. 2018. PMID: 30326051 No abstract available.
-
Magnetic Resonance Imaging-Based Prediction of Prostate Cancer Risk-Reply.JAMA Oncol. 2018 Nov 1;4(11):1625. doi: 10.1001/jamaoncol.2018.4234. JAMA Oncol. 2018. PMID: 30326079 No abstract available.
References
-
- Schröder FH, Hugosson J, Roobol MJ, et al. ; ERSPC Investigators . Screening and prostate-cancer mortality in a randomized European study. N Engl J Med. 2009;360(13):1320-1328. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7-30. - PubMed
-
- Borghesi M, Ahmed H, Nam R, et al. Complications after systematic, random, and image-guided prostate biopsy. Eur Urol. 2017;71(3):353-365. - PubMed
-
- Mottet N, Bellmunt J, Bolla M, et al. EAU-ESTRO-SIOG guidelines on prostate cancer, part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2017;71(4):618-629. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
