

Sacral neuromodulation versus personalized conservative treatment in patients with idiopathic slow-transit constipation: study protocol of the No.2-trial, a multicenter open-label randomized controlled trial and cost-effectiveness analysis
- PMID: 29470731
- PMCID: PMC5859034
- DOI: 10.1007/s00384-018-2978-x
Sacral neuromodulation versus personalized conservative treatment in patients with idiopathic slow-transit constipation: study protocol of the No.2-trial, a multicenter open-label randomized controlled trial and cost-effectiveness analysis
Abstract
Purpose: The evidence regarding the (cost-)effectiveness of sacral neuromodulation (SNM) in patients with therapy-resistant idiopathic slow-transit constipation is of suboptimal quality. The Dutch Ministry of Health, Welfare and Sports has granted conditional reimbursement for SNM treatment. The objective is to assess the effectiveness, cost-effectiveness, and budget impact of SNM compared to personalized conservative treatment (PCT) in patients with idiopathic slow-transit constipation refractory to conservative treatment.
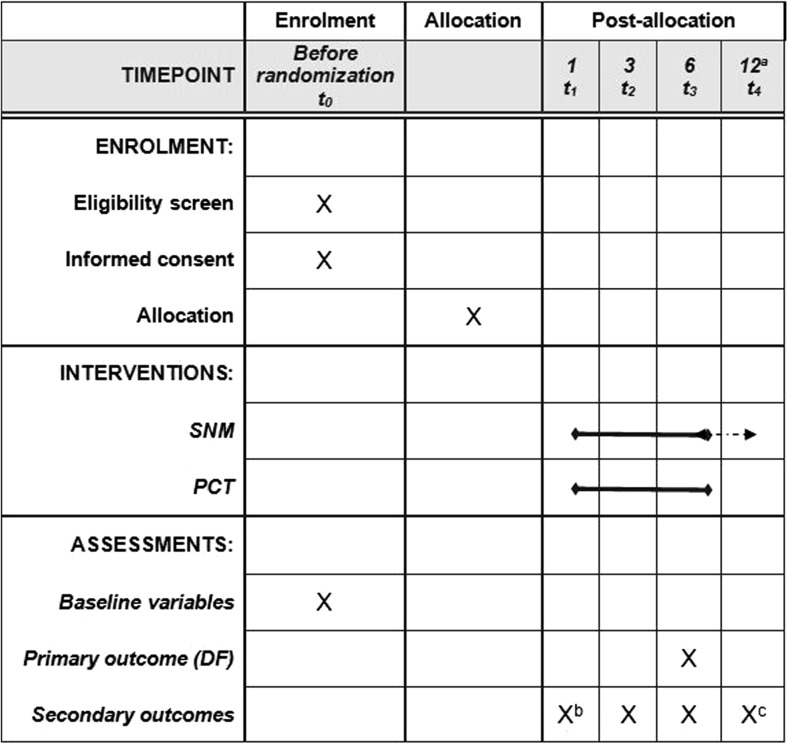
Methods: This study is an open-label, multicenter randomized controlled trial. Patients aged 14 to 80 with slow-transit constipation, a defecation frequency (DF) < 3 per week and meeting at least one other Rome-IV criterion, are eligible. Patients with obstructed outlet, irritable bowel syndrome, bowel pathology, or rectal prolapse are excluded. Patients are randomized to SNM or PCT. The primary outcome is success at 6 months (DF ≥ 3 a week), requiring a sample size of 64 (α = 0.05, β = 0.80, 30% difference in success). Secondary outcomes are straining, sense of incomplete evacuation, constipation severity, fatigue, constipation specific and generic quality of life, and costs at 6 months. Long-term costs and effectiveness will be estimated by a decision analytic model. The time frame is 57 months, starting October 2016. SNM treatment costs are funded by the Dutch conditional reimbursement program, research costs by Medtronic.
Conclusions: The results of this trial will be used to make a final decision regarding reimbursement of SNM from the Dutch Health Care Package in this patient group.
Trial registration: This trial is registered at clinicaltrials.gov , identifier NCT02961582, on 12 October 2016.
Keywords: Constipation; Cost-effectiveness; Quality of life; Sacral neuromodulation.
Conflict of interest statement
Competing interests
SOB and JM receive an unrestricted grant from Medtronic. The grant provided by Medtronic is partially used for the employment of SCMH. MAB is consultant for Shire, Sucampo, Coloplast, and Norgin.
Ethics approval and informed consent
The study will be conducted according to the principles of the 1964 Declaration of Helsinki and its later amendments, and in accordance with the Medical Research Involving Human Subjects Act. The study protocol has been approved by the Medical Ethical Committee of the Maastricht University Medical Center/Maastricht University in Maastricht, the Netherlands (METC161044). Written informed consent will be obtained from all participants included in the study, after a screening, and receiving, reading, and discussing the participant information brochure with the researcher. Consent will take place prior to randomization.
Figures

References
-
- Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M. Childhood functional gastrointestinal disorders: child/adolescent. Gastroenterology. 2016;150(6):1456–1468. doi: 10.1053/j.gastro.2016.02.015. - DOI
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
