

Not seeking yet trying long-acting reversible contraception: a 24-month randomized trial on continuation, unintended pregnancy and satisfaction
- PMID: 29470950
- PMCID: PMC6331179
- DOI: 10.1016/j.contraception.2018.02.001
Not seeking yet trying long-acting reversible contraception: a 24-month randomized trial on continuation, unintended pregnancy and satisfaction
Abstract
Objectives: To measure the 24-month impact on continuation, unintended pregnancy and satisfaction of trying long-acting reversible contraception (LARC) in a population seeking short-acting reversible contraception (SARC).
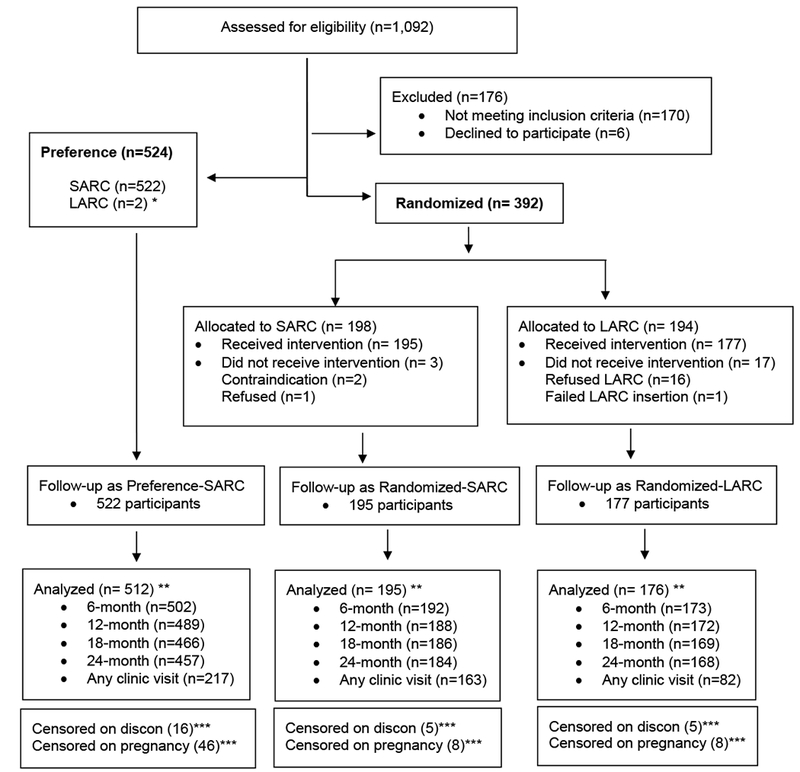
Study design: We enrolled 916 women aged 18-29 who were seeking pills or injectables in a partially randomized patient preference trial. Women with strong preferences for pills or injectables started on those products, while others opted for randomization to LARC or SARC and received their methods gratis. We estimated continuation and unintended pregnancy rates through 24months. Intent-to-treat principles were applied after method initiation for comparing incidence of unintended pregnancy. We also examined how satisfaction levels varied by cohort and how baseline negative LARC attitudes were associated with satisfaction over time.
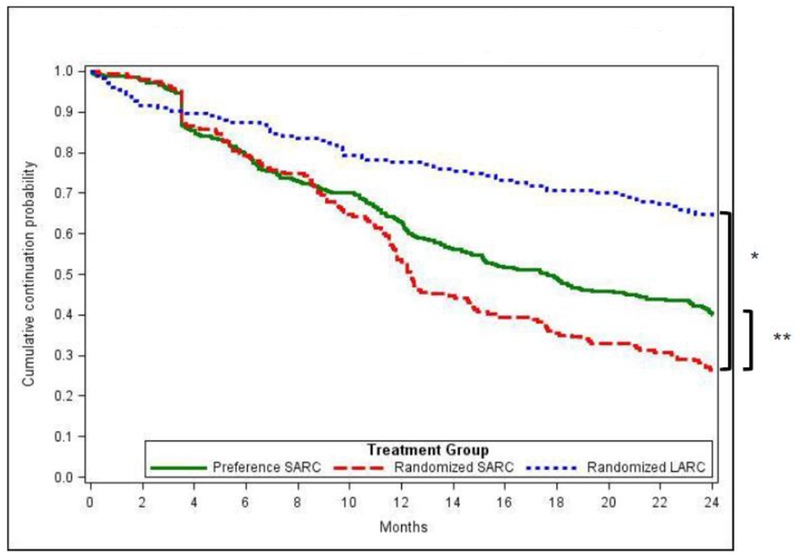
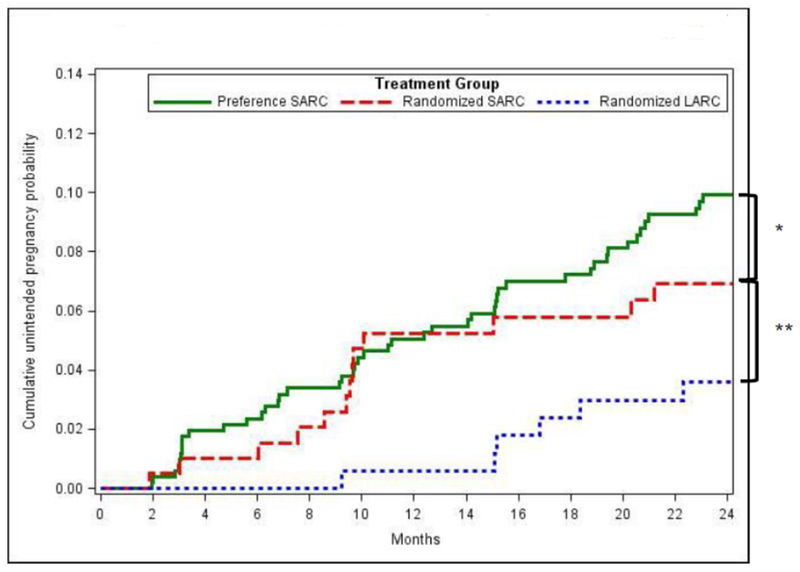
Results: Forty-three percent chose randomization, and 57% chose the preference option. Complete loss to follow-up was<2%. The 24-month LARC continuation probability was 64.3% [95% confidence interval (CI): 56.6-70.9], statistically higher than SARC groups [25.5% (randomized) and 40.0% (preference)]. The 24-month cumulative unintended pregnancy probabilities were 9.9% (95% CI: 7.2-12.6) (preference-SARC), 6.9% (95% CI: 3.3-10.6) (randomized-SARC) and 3.6% (95% CI: 1.8-6.4) (randomized-LARC). Statistical tests for comparing randomized groups on unintended pregnancy were mixed: binomial at 24-month time point (p=.02) and log-rank survival probabilities (p=.14 for first pregnancies and p=.07 when including second pregnancies). LARC satisfaction was high (80% happy/neutral, 73% would use LARC again, 81% would recommend to a friend). Baseline negative attitudes toward LARC (27%) were not clearly associated with satisfaction or early discontinuation.
Conclusions: The decision to try LARC resulted in high continuation rates and substantial protection from unintended pregnancy over 24months. Despite participants' initial desires to begin short-acting regimens, they had high satisfaction with LARC. Voluntary decisions to try LARC will benefit large proportions of typical SARC users.
Implications: Even women who do not necessarily view LARC as a first choice may have a highly satisfying experience and avoid unintended pregnancy if they try it.
Trial registration: ClinicalTrials.gov NCT01299116.
Keywords: Acceptability, contraceptive continuation; Adherence; Long-acting reversible contraception; Randomized; Unintended pregnancy.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
The remaining authors report no potential conflicts of interest.
Figures
References
-
- Daniels K, Daugherty J, Jones J, Mosher W. Current Contraceptive Use and Variation by Selected Characteristics Among Women Aged 15-44: United States, 2011-2013. Natl Health Stat Report. 2015:1–14. - PubMed
-
- Winner B, Peipert JF, Zhao Q, et al. Effectiveness of long-acting reversible contraception. The New England journal of medicine. 2012;366:1998–2007. - PubMed
-
- CDC. Centers for Disease Control Prevention. Contraceptive methods available to patients of office-based physicians and title X clinics — United States, 2009–2010. MMWR Morbidity and mortality weekly report. 2011;60:1–4. - PubMed
-
- Foster DG, Barar R, Gould H, Gomez I, Nguyen D, Biggs MA. Projections and opinions from 100 experts in long-acting reversible contraception. Contraception. 2015;92:543–52. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
