

Reverse Myocardial Remodeling Following Valve Replacement in Patients With Aortic Stenosis
- PMID: 29471937
- PMCID: PMC5821681
- DOI: 10.1016/j.jacc.2017.12.035
Reverse Myocardial Remodeling Following Valve Replacement in Patients With Aortic Stenosis
Abstract
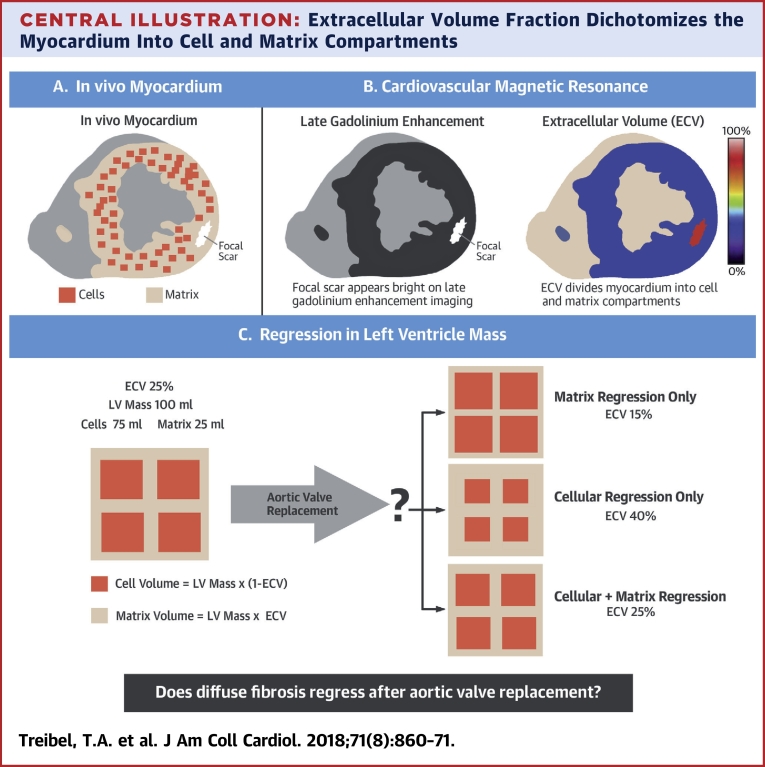
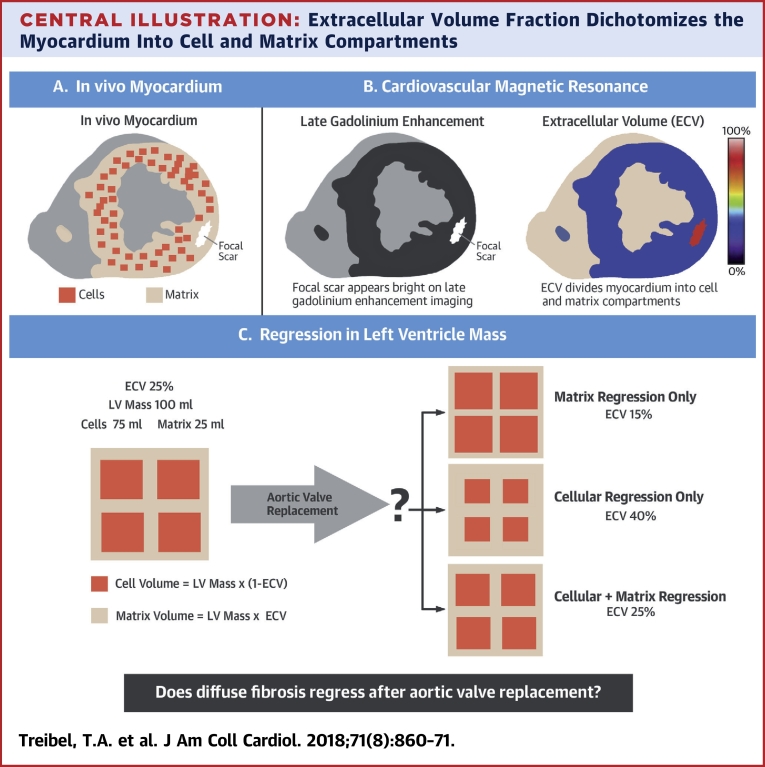
Background: Left ventricular (LV) hypertrophy, a key process in human cardiac disease, results from cellular (hypertrophy) and extracellular matrix expansion (interstitial fibrosis).
Objectives: This study sought to investigate whether human myocardial interstitial fibrosis in aortic stenosis (AS) is plastic and can regress.
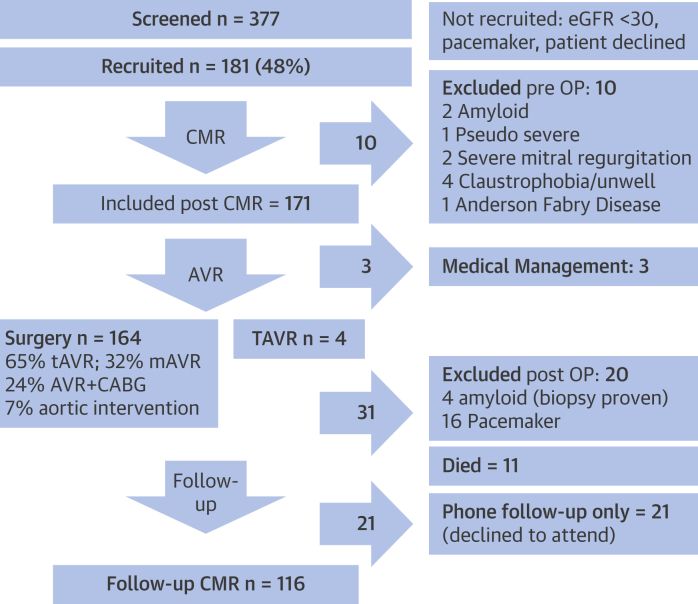
Methods: Patients with symptomatic, severe AS (n = 181; aortic valve area index 0.4 ± 0.1 cm2/m2) were assessed pre-aortic valve replacement (AVR) by echocardiography (AS severity, diastology), cardiovascular magnetic resonance (CMR) (for volumes, function, and focal or diffuse fibrosis), biomarkers (N-terminal pro-B-type natriuretic peptide and high-sensitivity troponin T), and the 6-min walk test. CMR was used to measure the extracellular volume fraction (ECV), thereby deriving matrix volume (LV mass × ECV) and cell volume (LV mass × [1 - ECV]). Biopsy excluded occult bystander disease. Assessment was repeated at 1 year post-AVR.
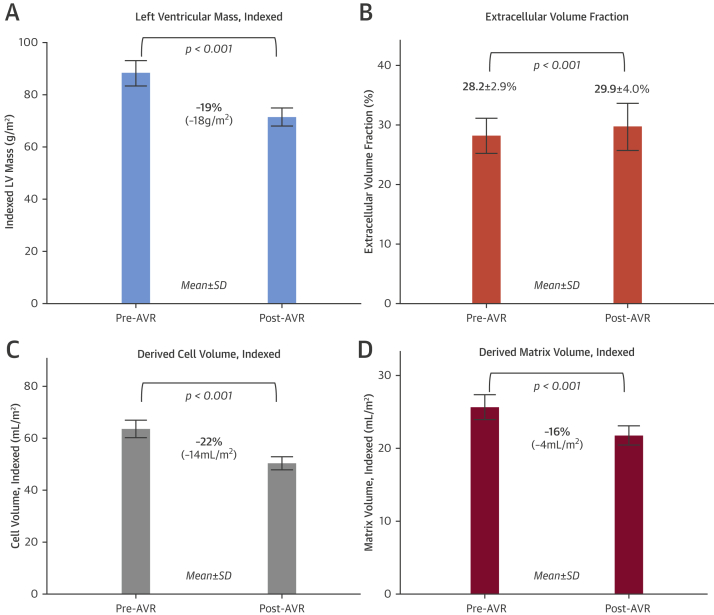
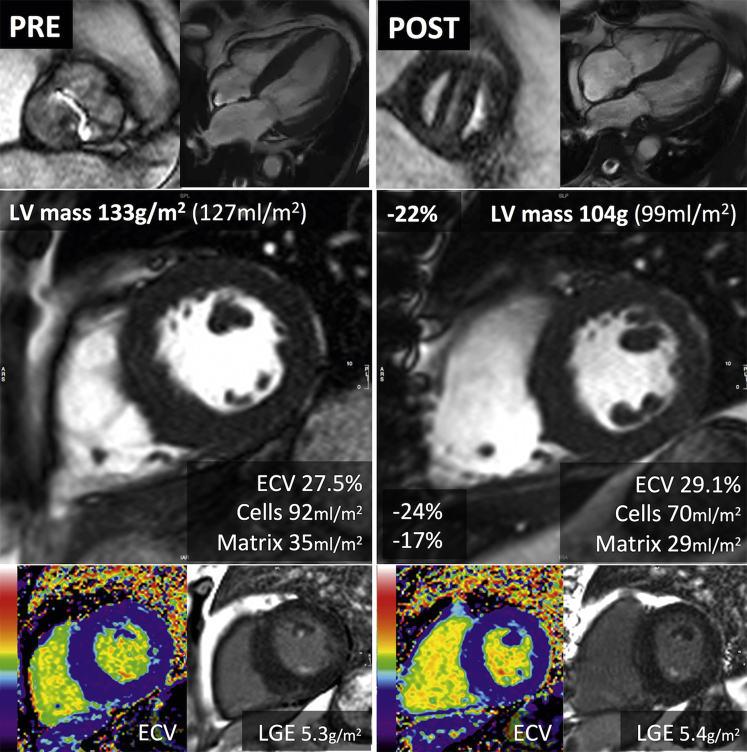
Results: At 1 year post-AVR in 116 pacemaker-free survivors (age 70 ± 10 years; 54% male), mean valve gradient had improved (48 ± 16 mm Hg to 12 ± 6 mm Hg; p < 0.001), and indexed LV mass had regressed by 19% (88 ± 26 g/m2 to 71 ± 19 g/m2; p < 0.001). Focal fibrosis by CMR late gadolinium enhancement did not change, but ECV increased (28.2 ± 2.9% to 29.9 ± 4.0%; p < 0.001): this was the result of a 16% reduction in matrix volume (25 ± 9 ml/m2 to 21 ± 7 ml/m2; p < 0.001) but a proportionally greater 22% reduction in cell volume (64 ± 18 ml/m2 to 50 ± 13 ml/m2; p < 0.001). These changes were accompanied by improvement in diastolic function, N-terminal pro-B-type natriuretic peptide, 6-min walk test results, and New York Heart Association functional class.
Conclusions: Post-AVR, focal fibrosis does not resolve, but diffuse fibrosis and myocardial cellular hypertrophy regress. Regression is accompanied by structural and functional improvements suggesting that human diffuse fibrosis is plastic, measurable by CMR and a potential therapeutic target. (Regression of Myocardial Fibrosis After Aortic Valve Replacement; NCT02174471).
Keywords: aortic stenosis; fibrosis; left ventricular hypertrophy.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Revisiting Reverse Remodeling After Aortic Valve Replacement for Aortic Stenosis.J Am Coll Cardiol. 2018 Feb 27;71(8):872-874. doi: 10.1016/j.jacc.2017.12.036. J Am Coll Cardiol. 2018. PMID: 29471938 No abstract available.
-
Reply: Aortic Stenosis, Left Ventricular Remodeling, and Renin-Angiotensin System Blockade.J Am Coll Cardiol. 2018 Jun 26;71(25):2984-2985. doi: 10.1016/j.jacc.2018.04.034. J Am Coll Cardiol. 2018. PMID: 29929624 No abstract available.
-
Aortic Stenosis, Left Ventricular Remodeling, and Renin-Angiotensin System Blockade.J Am Coll Cardiol. 2018 Jun 26;71(25):2984. doi: 10.1016/j.jacc.2018.02.084. J Am Coll Cardiol. 2018. PMID: 29929625 No abstract available.
References
-
- Nkomo V.T., Gardin J.M., Skelton T.N., Gottdiener J.S., Scott C.G., Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–1011. - PubMed
-
- Houser S.R., Margulies K.B., Murphy A.M. Animal models of heart failure: a scientific statement from the American Heart Association. Circ Res. 2012;111:131–150. - PubMed
-
- Azevedo C.F., Nigri M., Higuchi M.L. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J Am Coll Cardiol. 2010;56:278–287. - PubMed
-
- Dweck M.R., Joshi S., Murigu T. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. J Am Coll Cardiol. 2011;58:1271–1279. - PubMed
-
- Barone-Rochette G., Pierard S., De Meester de Ravenstein C. Prognostic significance of LGE by CMR in aortic stenosis patients undergoing valve replacement. J Am Coll Cardiol. 2014;64:144–154. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
