

doi: 10.1212/CPJ.0b013e3182a1b9bd.
Neurologic complications of anesthesia: A practical approach
Affiliations
- PMID: 29473613
- PMCID: PMC5765958
- DOI: 10.1212/CPJ.0b013e3182a1b9bd
Item in Clipboard
Neurologic complications of anesthesia: A practical approach
Neurol Clin Pract.
2013 Aug.
Abstract
Neurologic complications related to anesthesia are infrequent but can be serious. Neurologists are often consulted to evaluate patients with postoperative symptoms and must be ready to discriminate those truly caused by the anesthetic drug or procedure from the more common postoperative complications that are unrelated to the anesthesia itself. This practical review relies on cases to illustrate common reasons for neurologic consultation in the postsurgical setting. It also briefly summarizes what to expect when patients with central or peripheral neurologic disease undergo surgery under general or regional anesthesia.
Figures
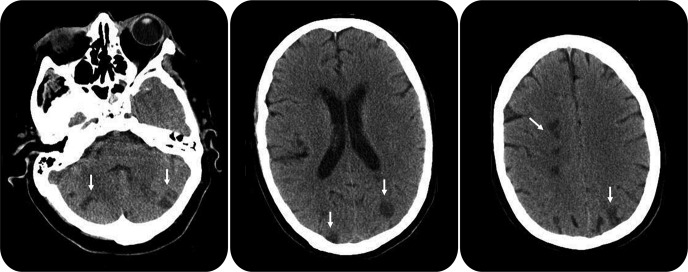
Perioperative brain infarctions Figure 1. Noncontrast head CT scan of the patient described in vignette 2 shows multiple embolic infarctions (arrows).
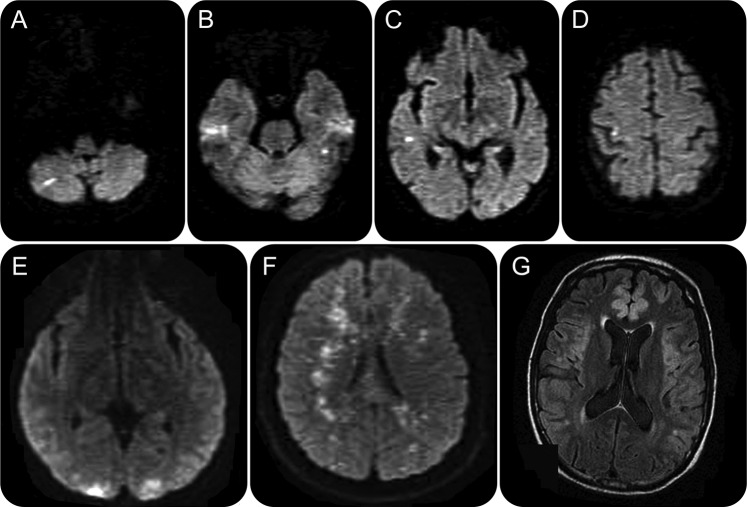
Value of MRI of the brain in patients with altered consciousness after surgery Figure 2. (A–D) Diffusion-weighted imaging (DWI) sequence of a patient with multiple small infarctions caused by an embolic shower, which could not be visualized on CT scan. (E) DWI of a patient with top-of-the-basilar syndrome diagnosed after a cardiovascular procedure. He recovered consciousness but had persistent bilateral visual loss from bilateral occipital infarctions. (F) DWI of a patient with fat embolism after repair of a complex long bone fracture shows the typical “star-field appearance.” (G) Fluid-attenuated inversion recovery sequence of a patient with severe cortical laminar necrosis after an emergency vascular surgery preceded by profound hypoxia and shock and complicated by refractory intraoperative hypotension.
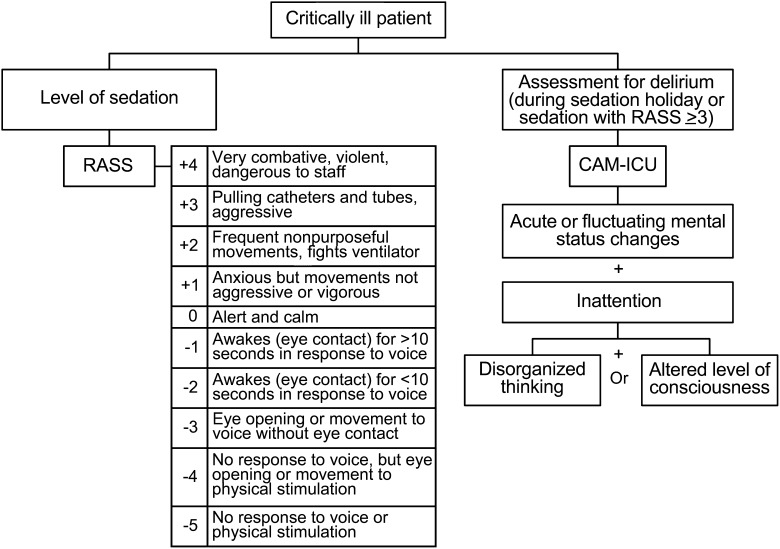
Sedation and delirium assessment tools Figure 3. Evaluation of level of sedation and delirium using the Richmond Agitation Sedation Scale (RASS) and Confusion Assessment Method for the Intensive Care Unit (CAM-ICU).
Similar articles
-
Effectiveness of ondansetron as an adjunct to lidocaine intravenous regional anesthesia on tourniquet pain and postoperative pain in patients undergoing elective hand surgery: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):27-38. doi: 10.11124/jbisrir-2015-1768. JBI Database System Rev Implement Rep. 2015. PMID: 26447005
-
Neurologic issues and obstetric anesthesia.Semin Neurol. 2011 Sep;31(4):374-84. doi: 10.1055/s-0031-1293536. Epub 2011 Nov 23. Semin Neurol. 2011. PMID: 22113509 Review.
-
Incidence of local anesthetic systemic toxicity and postoperative neurologic symptoms associated with 12,668 ultrasound-guided nerve blocks: an analysis from a prospective clinical registry.Reg Anesth Pain Med. 2012 Sep-Oct;37(5):478-82. doi: 10.1097/AAP.0b013e31825cb3d6. Reg Anesth Pain Med. 2012. PMID: 22705953
-
[Forefoot surgery under regional anesthesia].Acta Chir Orthop Traumatol Cech. 2005;72(2):122-4. Acta Chir Orthop Traumatol Cech. 2005. PMID: 15890145 Czech.
-
[Anesthesia procedures--postoperative effects].Anaesthesist. 1997 Oct;46 Suppl 2:S99-108. doi: 10.1007/pl00002480. Anaesthesist. 1997. PMID: 9432882 Review. German.
Cited by
-
Movement Disorders Associated With Radiotherapy and Surgical Procedures.J Mov Disord. 2023 Jan;16(1):42-51. doi: 10.14802/jmd.22092. Epub 2023 Jan 12. J Mov Disord. 2023. PMID: 36628430 Free PMC article.
-
Anesthetic Considerations in Athletes: A Review.Cureus. 2025 Mar 23;17(3):e81040. doi: 10.7759/cureus.81040. eCollection 2025 Mar. Cureus. 2025. PMID: 40271321 Free PMC article. Review.
-
Hepatic Encephalopathy: From Metabolic to Neurodegenerative.Neurochem Res. 2021 Oct;46(10):2612-2625. doi: 10.1007/s11064-021-03372-4. Epub 2021 Jun 15. Neurochem Res. 2021. PMID: 34129161 Review.
-
Postoperative Neurological Deficits Following Regional Anesthesia: A Rare Case of Transient Aphasia and Hemiparesis.Cureus. 2025 Apr 9;17(4):e81953. doi: 10.7759/cureus.81953. eCollection 2025 Apr. Cureus. 2025. PMID: 40351973 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources