

Temporal Trends in Incidence, Sepsis-Related Mortality, and Hospital-Based Acute Care After Sepsis
- PMID: 29474320
- PMCID: PMC5896750
- DOI: 10.1097/CCM.0000000000002872
Temporal Trends in Incidence, Sepsis-Related Mortality, and Hospital-Based Acute Care After Sepsis
Abstract
Objectives: A growing number of patients survive sepsis hospitalizations each year and are at high risk for readmission. However, little is known about temporal trends in hospital-based acute care (emergency department treat-and-release visits and hospital readmission) after sepsis. Our primary objective was to measure temporal trends in sepsis survivorship and hospital-based acute care use in sepsis survivors. In addition, because readmissions after pneumonia are subject to penalty under the national readmission reduction program, we examined whether readmission rates declined after sepsis hospitalizations related to pneumonia.
Design and setting: Retrospective, observational cohort study conducted within an academic healthcare system from 2010 to 2015.
Patients: We used three validated, claims-based approaches to identify 17,256 sepsis or severe sepsis hospitalizations to examine trends in hospital-based acute care after sepsis.
Interventions: None.
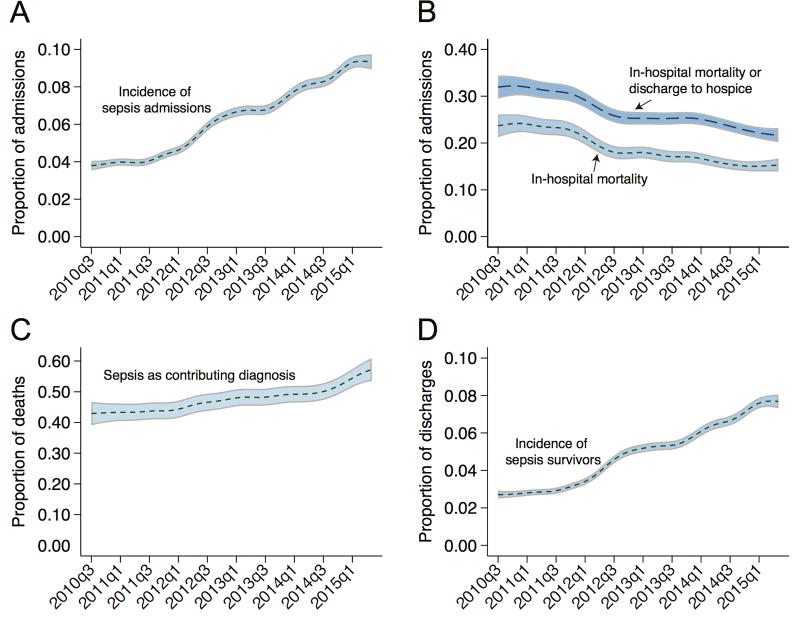
Measurements and main results: From 2010 to 2015, sepsis as a proportion of medical and surgical admissions increased from 3.9% to 9.4%, whereas in-hospital mortality rate for sepsis hospitalizations declined from 24.1% to 14.8%. As a result, the proportion of medical and surgical discharges at-risk for hospital readmission after sepsis increased from 2.7% to 7.8%. Over 6 years, 30-day hospital readmission rates declined modestly, from 26.4% in 2010 to 23.1% in 2015, driven largely by a decline in readmission rates among survivors of nonsevere sepsis, and nonpneumonia sepsis specifically, as the readmission rate of severe sepsis survivors was stable. The modest decline in 30-day readmission rates was offset by an increase in emergency department treat-and-release visits, from 2.8% in 2010 to a peak of 5.4% in 2014.
Conclusions: Owing to increasing incidence and declining mortality, the number of sepsis survivors at risk for hospital readmission rose significantly between 2010 and 2015. The 30-day hospital readmission rates for sepsis declined modestly but were offset by a rise in emergency department treat-and-release visits.
Conflict of interest statement
For each of the above authors, no financial or other potential conflicts of interest exist related to the work.
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–10. - PubMed
-
- Gaieski DF, Edwards JM, Kallans MJ, et al. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med. 2013;41:1167–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
