

Support surfaces for pressure ulcer prevention: A network meta-analysis
- PMID: 29474359
- PMCID: PMC5825032
- DOI: 10.1371/journal.pone.0192707
Support surfaces for pressure ulcer prevention: A network meta-analysis
Abstract
Background: Pressure ulcers are a prevalent and global issue and support surfaces are widely used for preventing ulceration. However, the diversity of available support surfaces and the lack of direct comparisons in RCTs make decision-making difficult.
Objectives: To determine, using network meta-analysis, the relative effects of different support surfaces in reducing pressure ulcer incidence and comfort and to rank these support surfaces in order of their effectiveness.
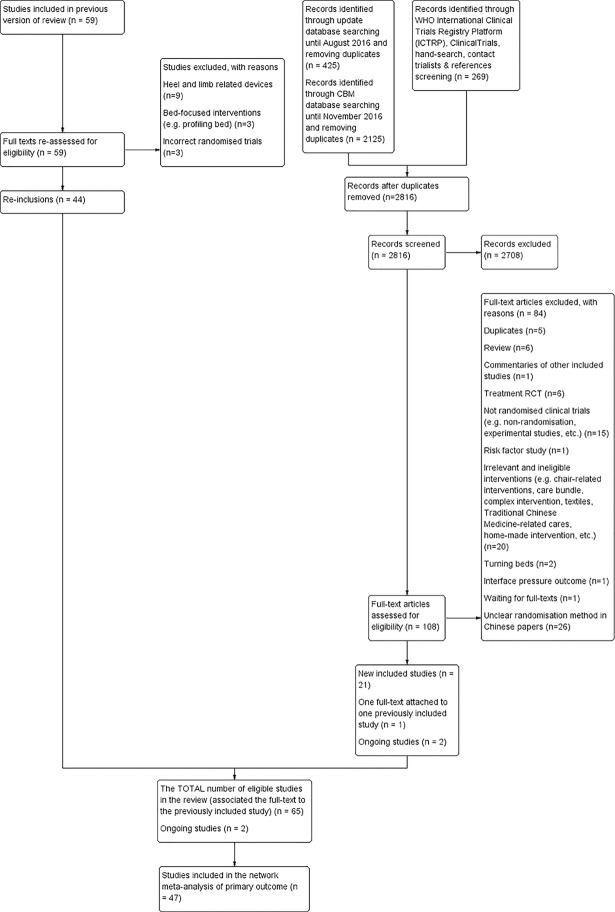
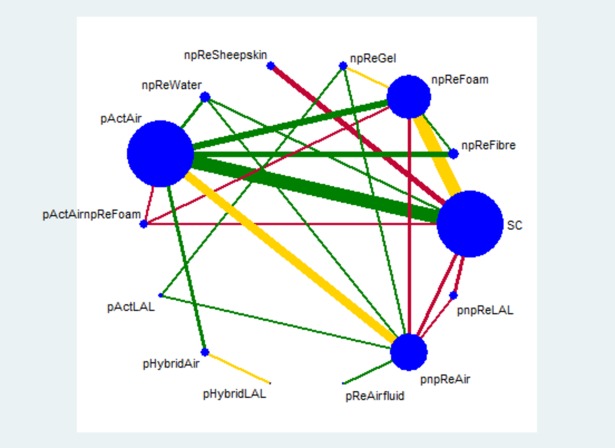
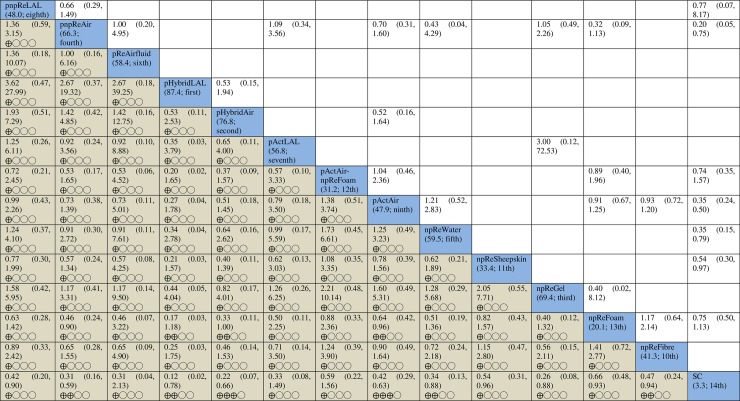
Methods: We conducted a systematic review, using a literature search up to November 2016, to identify randomised trials comparing support surfaces for pressure ulcer prevention. Two reviewers independently performed study selection, risk of bias assessment and data extraction. We grouped the support surfaces according to their characteristics and formed evidence networks using these groups. We used network meta-analysis to estimate the relative effects and effectiveness ranking of the groups for the outcomes of pressure ulcer incidence and participant comfort. GRADE was used to assess the certainty of evidence.
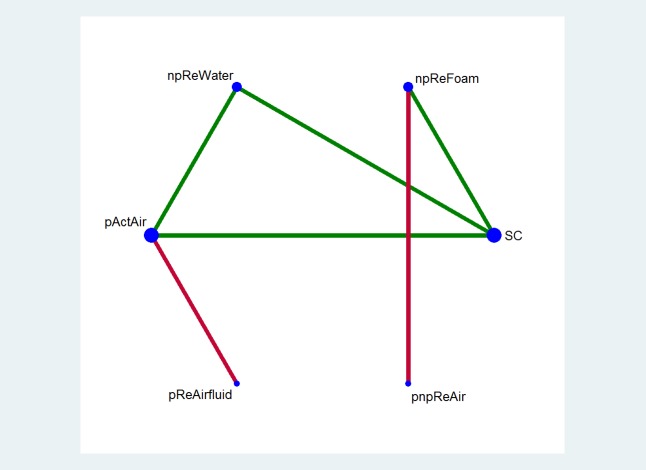
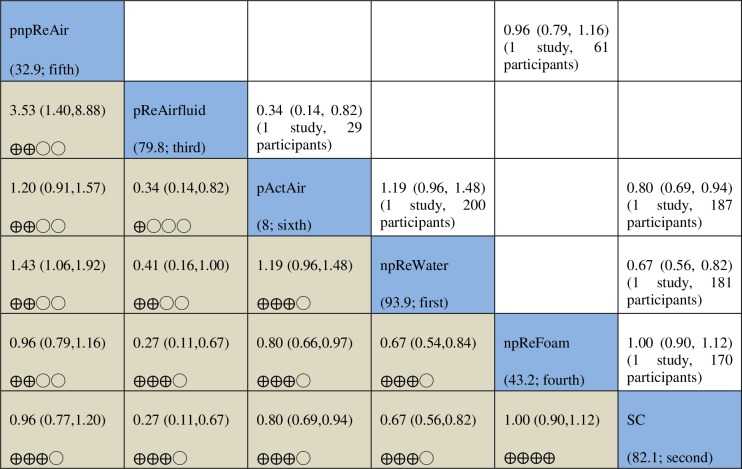
Main results: We included 65 studies in the review. The network for assessing pressure ulcer incidence comprised evidence of low or very low certainty for most network contrasts. There was moderate-certainty evidence that powered active air surfaces and powered hybrid air surfaces probably reduce pressure ulcer incidence compared with standard hospital surfaces (risk ratios (RR) 0.42, 95% confidence intervals (CI) 0.29 to 0.63; 0.22, 0.07 to 0.66, respectively). The network for comfort suggested that powered active air-surfaces are probably slightly less comfortable than standard hospital mattresses (RR 0.80, 95% CI 0.69 to 0.94; moderate-certainty evidence).
Conclusions: This is the first network meta-analysis of the effects of support surfaces for pressure ulcer prevention. Powered active air-surfaces probably reduce pressure ulcer incidence, but are probably less comfortable than standard hospital surfaces. Most prevention evidence was of low or very low certainty, and more research is required to reduce these uncertainties.
Conflict of interest statement
Figures
References
-
- National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (NPUAP/EPUAP/PPPIA). Prevention and Treatment of Pressure Ulcers: Quick Reference Guide. Haesler Emily (Ed.). Cambridge Media: Osborne Park, Western Australia; 2014.
-
- Cullum N, Buckley H, Dumville J, Hall J, Lamb K, Madden M, et al. Wounds research for patient benefit: a 5-year programme of research, Programme Grants for Applied Research. NIHR Journals Library, Southampton (UK); 2016. - PubMed
-
- Bennett G, Dealey C, Posnett J. The cost of pressure ulcers in the UK. Age Ageing 2004; 33: 230–235. doi: 10.1093/ageing/afh086 - DOI - PubMed
-
- National Pressure Ulcer Advisory Panel (NPUAP). Support Surface Standards (S3I) Terms and Definitions Related to Support Surfaces. Available at http://www.npuap.org/wp-content/uploads/2012/03/NPUAP_S3I_TD.pdf Access in 15 Dec. 15.
-
- Clark M. Technology update: understanding support surface. Wounds International 2011; 2(3):17–21.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
