

Acute liver failure in children-Is living donor liver transplantation justified?
- PMID: 29474400
- PMCID: PMC5825073
- DOI: 10.1371/journal.pone.0193327
Acute liver failure in children-Is living donor liver transplantation justified?
Abstract
Objectives: Living donor liver transplantation (LDLT) in patients with acute liver failure (ALF) has become an acceptable alternative to transplantation from deceased donors (DDLT). The aim of this study was to analyze outcomes of LDLT in pediatric patients with ALF based on our center's experience.
Material and methods: We enrolled 63 children (at our institution) with ALF who underwent liver transplantation between 1997 and 2016. Among them 24 (38%) underwent a LDLT and 39 (62%) received a DDLT. Retrospectively analyzed patient clinical data included: time lapse between qualification for transplantation and transplant surgery, graft characteristics, postoperative complications, long-term results post-transplantation, and living donor morbidity. Overall, we have made a comparison of clinical results between LDLT and DDLT groups.
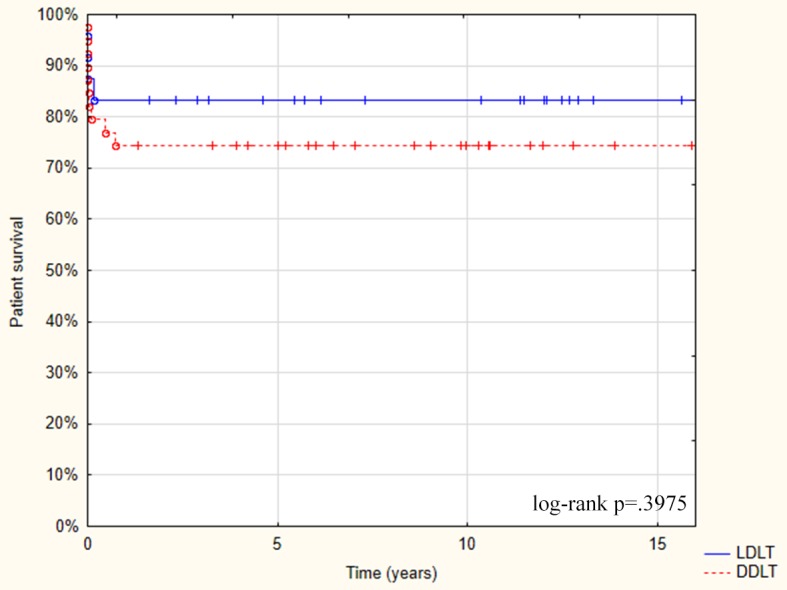
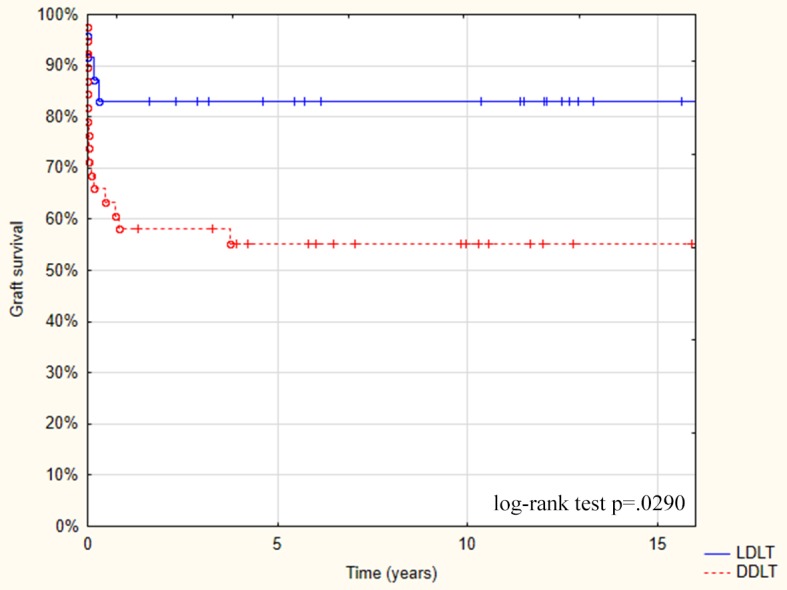
Results: Follow-up periods ranged from 12 to 182 months (median 109 months) for LDLT patients and 12 to 183 months (median 72 months) for DDLT patients. The median waiting time for a transplant was shorter in LDLT group than in DDLT group. There was not a single case of primary non-function (PNF) in the LDLT group and 20 out of 24 patients (83.3%) had good early graft function; 3 patients (12.5%) in the LDLT group died within 2 months of transplantation but there was no late mortality. In comparison, 4 out of 39 patients (10.2%) had PNF in DDLT group while 20 patients (51.2%) had good early graft function; 8 patients (20.5%) died early within 2 months and 2 patients (5.1%) died late after transplantation. The LDLT group had a shorter cold ischemia time (CIT) of 4 hours in comparison to 9.2 hours in the DDLT group (p<0.0001).
Conclusions: LDLT is a lifesaving procedure for pediatric patients with ALF. Our experience showed that it may be performed with very good results, and with very low morbidity and no mortality among living donors when performed by experienced teams following strict procedures.
Conflict of interest statement
Figures
References
-
- Trey C, Dawidson CS. The management of fulminant hepatic failure In: Popper H, Schaffner F, editors. Progress in Liver Diseases. Volume 3. New York: Grune&Stratton; 1970. pp. 282–98. - PubMed
-
- Bhaduri B, Mieli -Vergani G. Fulminant hepatic failure: pediatric aspects. Semin Liv Dis. 1996; 16: 349–355. - PubMed
-
- Lutfi R, Abulebda K, Nitu ME, Molleston JP, Bozic MA, Subbarao G. Intensive Care Management of Pediatric Acute Failure. J Pediatr Gastroenterol Nutr. 2017; 64, 5: 660–670. doi: 10.1097/MPG.0000000000001441 - DOI - PubMed
-
- Jain V, Dhavan A. Prognostic Modeling in Pediatric Acute Liver Failure. Liver Transpl. 2016; 22, 10: 1418–1430. doi: 10.1002/lt.24501 - DOI - PubMed
-
- Matsunami H, Makuuchi M, Kawasaki S, Ishizone S, Mizusawa Y, Kawarasaki H, et al. Living-related liver transplantation in fulminant hepatic failure. Lancet. 1992; 340, 8832: 1411–12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
