

Predicting excess cost for older inpatients with clinical complexity: A retrospective cohort study examining cognition, comorbidities and complications
- PMID: 29474407
- PMCID: PMC5825075
- DOI: 10.1371/journal.pone.0193319
Predicting excess cost for older inpatients with clinical complexity: A retrospective cohort study examining cognition, comorbidities and complications
Abstract
Background: Hospital-acquired complications increase length of stay and contribute to poorer patient outcomes. Older adults are known to be at risk for four key hospital-acquired complications (pressure injuries, pneumonia, urinary tract infections and delirium). These complications have been identified as sensitive to nursing characteristics such as staffing levels and level of education. The cost of these complications compared to the cost of admission severity, dementia, other comorbidities or age has not been established.
Method: To investigate costs associated with nurse-sensitive hospital-acquired complications in an older patient population 157,178 overnight public hospital episodes for all patients over age 50 from one Australian state, 2006/07 were examined. A retrospective cohort study design with linear regression analysis provided modelling of length-of-stay costs. Explanatory variables included patient age, sex, comorbidities, admission severity, dementia status, surgical status and four complications. Extra costs were based on above-average length-of-stay for each patient's Diagnosis Related Group from hospital discharge data.
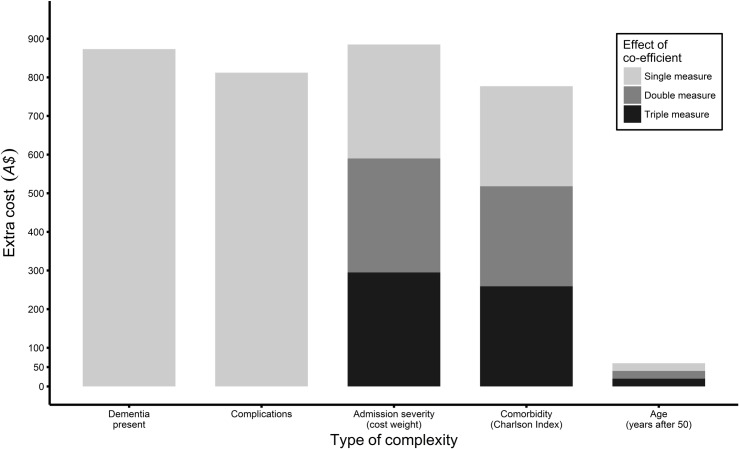
Results: For adults over 50 who have length of stay longer than average for their diagnostic condition, comorbid dementia predicts an extra cost of A$874, (US$1,247); any one of four key complications predicts A$812 (US$1,159); each increase in admission severity score predicts A$295 ($US421); each additional comorbidity predicts A$259 (US$370), and for each year of age above 50 predicts A$20 (US$29) (all estimates significant at p<0.0001).
Discussion: Hospital-acquired complications and dementia cost more than other kinds of inpatient complexity, but admission severity is a better predictor of excess cost. Because complications are potentially preventable and dementia care in hospitals can be improved, risk-reduction strategies for common complications, particularly for patients with dementia could be cost effective.
Conclusions: Complications and dementia were found to cost more than other kinds of inpatient complexity.
Conflict of interest statement
References
-
- Kuo Y-F, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Annals of internal medicine. 2011;155(3):152–9. doi: 10.7326/0003-4819-155-3-201108020-00005 - DOI - PMC - PubMed
-
- Australian Institute of Health and Welfare. Australian hospital statistics 2011–12. Canberra: AIHW; 2013.
-
- Hickman L, Newton P, Halcomb EJ, Chang E, Davidson P. Best practice interventions to improve the management of older people in acute care settings: a literature review. Journal of Advanced Nursing. 2007;60(2):113–26. doi: 10.1111/j.1365-2648.2007.04417.x PubMed PMID: WOS:000249488100001. - DOI - PubMed
-
- Arora V, Chen S, Juned S, Sachs G, Meltzer D. Relationship between quality of care and functional decline for hospitalized vulnerable elders. Journal of the American Geriatrics Society. 2007;55(4):S198–S. PubMed PMID: WOS:000245752500582.
-
- Long SJ, Brown KF, Ames D, Vincent C. What is known about adverse events in older medical hospital inpatients? A systematic review of the literature. International Journal for Quality in Health Care. 2013;25(5):542–54. doi: 10.1093/intqhc/mzt056 PubMed PMID: WOS:000325501000007. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
