

Annual Burden and Costs of Hospitalization for High-Need, High-Cost Patients With Chronic Gastrointestinal and Liver Diseases
- PMID: 29474966
- PMCID: PMC6056327
- DOI: 10.1016/j.cgh.2018.02.015
Annual Burden and Costs of Hospitalization for High-Need, High-Cost Patients With Chronic Gastrointestinal and Liver Diseases
Abstract
Background & aims: We estimated the annual burden and costs of hospitalization in patients with chronic gastrointestinal and liver diseases, and identified characteristics of high-need, high-cost patients, in a nationally representative sample.
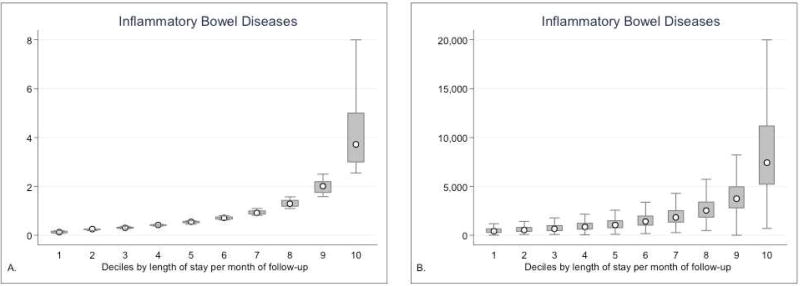
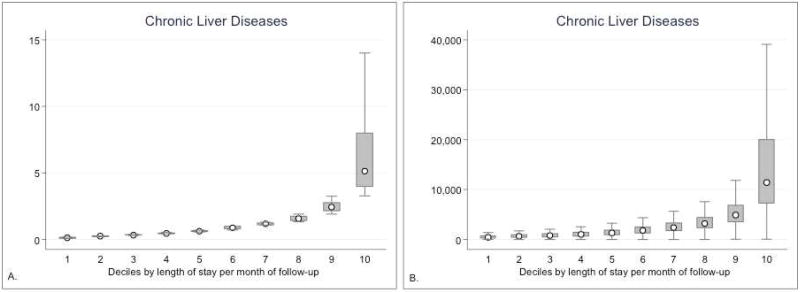
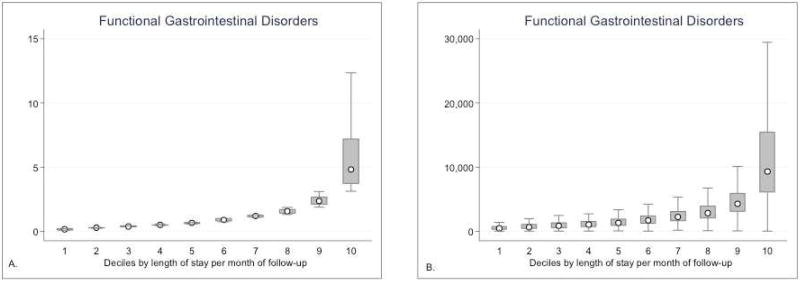
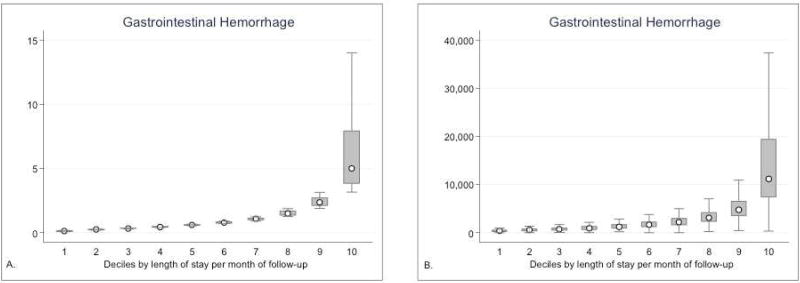
Methods: Using Nationwide Readmissions Database 2013, we identified patients with at least 1 hospitalization between January and June 2013, and a diagnosis of inflammatory bowel diseases (IBDs), chronic liver diseases (CLDs), functional gastrointestinal disorders (FGIDs), gastrointestinal hemorrhage, or pancreatic diseases, with 6 months or more of follow up. We calculated days spent in hospital/month and estimated costs of the entire cohort, and identified characteristics of high-need, high-cost patients (top decile of days spent in hospital/month).
Results: Patients with IBD (n = 47,402), CLDs (n = 376,810), FGIDs (n = 351,583), gastrointestinal hemorrhage (n = 190,881), or pancreatic diseases (n = 98,432), hospitalized at least once, spent a median of 6 to 7 days (interquartile range, 3-14 d) in the hospital each year (total for all diseases). Compared to patients in the lowest decile (median, 0.13-0.14 d/mo spent in the hospital), patients in the highest decile spent a median 3.7-4.1 days/month in hospital (total for all diseases), with hospitalization costs ranging from $7502/month to $8925/month and 1 hospitalization every 2 months. Gastrointestinal diseases, infections, and cardiopulmonary causes were leading reasons for hospitalization of these patients. Based on multivariate logistic regression, high-need, high-cost patients were more likely to have Medicare/Medicaid insurance, lower income status, index hospitalization in a large rural hospital, high comorbidity burden, obesity, and infection-related hospitalization.
Conclusions: In a nationwide database analysis of patients with IBD, CLD, FGID, gastrointestinal hemorrhage, or pancreatic diseases hospitalized at least once, we found that a small fraction of high-need, high-cost patients contribute disproportionately to hospitalization costs. Population health management directed toward these patients would facilitate high-value care.
Keywords: Health Care Spending; High Risk; Population Health Management; Utilization.
Copyright © 2018 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Boccuti CC, G . In: Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmissions Reduction Program. Foundation THJKF, editor. 2015.
-
- Thorpe JHC, T Medicare Hospital Readmissions Reduction Program. Legal Notes. 2011;3:1–4.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
