

A gene-expression profiling score for prediction of outcome in patients with follicular lymphoma: a retrospective training and validation analysis in three international cohorts
- PMID: 29475724
- PMCID: PMC5882539
- DOI: 10.1016/S1470-2045(18)30102-5
A gene-expression profiling score for prediction of outcome in patients with follicular lymphoma: a retrospective training and validation analysis in three international cohorts
Erratum in
-
Correction to Lancet Oncol 2018; 19: 549-61.Lancet Oncol. 2018 Jun;19(6):e283. doi: 10.1016/S1470-2045(18)30385-1. Epub 2018 Jun 1. Lancet Oncol. 2018. PMID: 29893260 No abstract available.
Abstract
Background: Patients with follicular lymphoma have heterogeneous outcomes. Predictor models to distinguish, at diagnosis, between patients at high and low risk of progression are needed. The objective of this study was to use gene-expression profiling data to build and validate a predictive model of outcome for patients treated in the rituximab era.
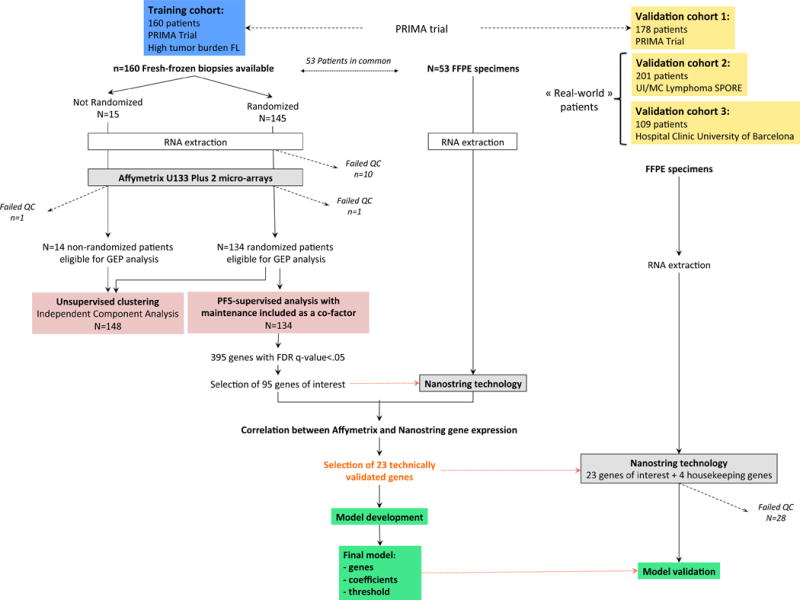
Methods: A training set of fresh-frozen tumour biopsies was prospectively obtained from 160 untreated patients with high-tumour-burden follicular lymphoma enrolled in the phase 3 randomised PRIMA trial, in which rituximab maintenance was evaluated after rituximab plus chemotherapy induction (median follow-up 6·6 years [IQR 6·0-7·0]). RNA of sufficient quality was obtained for 149 of 160 cases, and Affymetrix U133 Plus 2.0 microarrays were used for gene-expression profiling. We did a multivariate Cox regression analysis to identify genes with expression levels associated with progression-free survival independently of maintenance treatment in a subgroup of 134 randomised patients. Expression levels from 95 curated genes were then determined by digital expression profiling (NanoString technology) in 53 formalin-fixed paraffin-embedded samples of the training set to compare the technical reproducibility of expression levels for each gene between technologies. Genes with high correlation (>0·75) were included in an L2-penalised Cox model adjusted on rituximab maintenance to build a predictive score for progression-free survival. The model was validated using NanoString technology to digitally quantify gene expression in 488 formalin-fixed, paraffin-embedded samples from three independent international patient cohorts from the PRIMA trial (n=178; distinct from the training cohort), the University of Iowa/Mayo Clinic Lymphoma SPORE project (n=201), and the Barcelona Hospital Clinic (n=109). All tissue samples consisted of pretreatment diagnostic biopsies and were confirmed as follicular lymphoma grade 1-3a. The patients were all treated with regimens containing rituximab and chemotherapy, possibly followed by either rituximab maintenance or ibritumomab-tiuxetan consolidation. We determined an optimum threshold on the score to predict patients at low risk and high risk of progression. The model, including the multigene score and the threshold, was initially evaluated in the three validation cohorts separately. The sensitivity and specificity of the score for the prediction of the risk of lymphoma progression at 2 years were assessed on the combined validation cohorts.
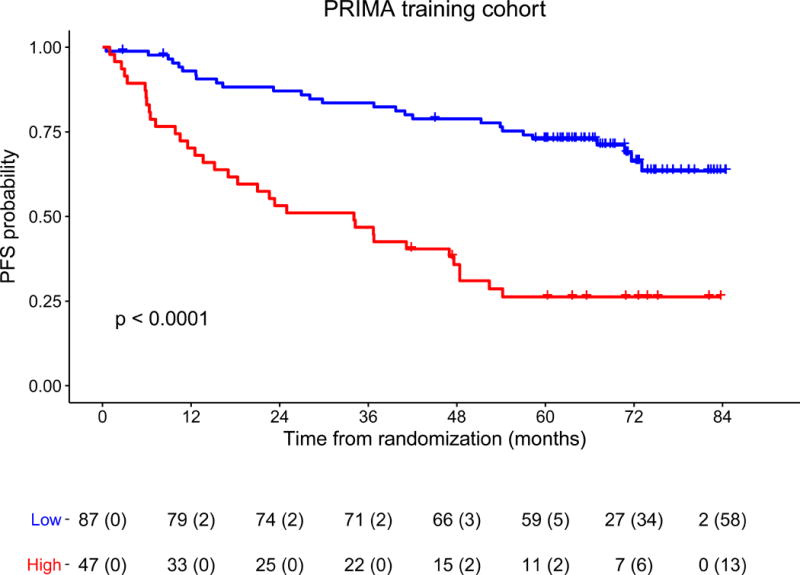
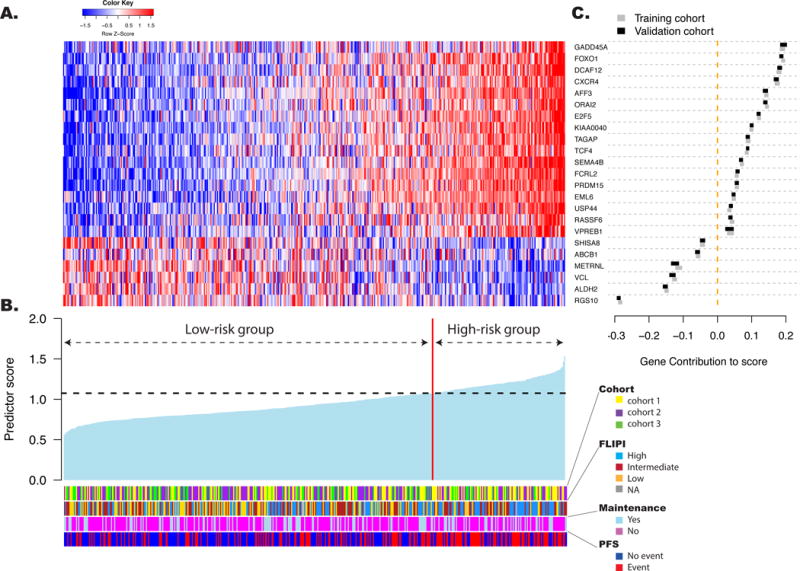
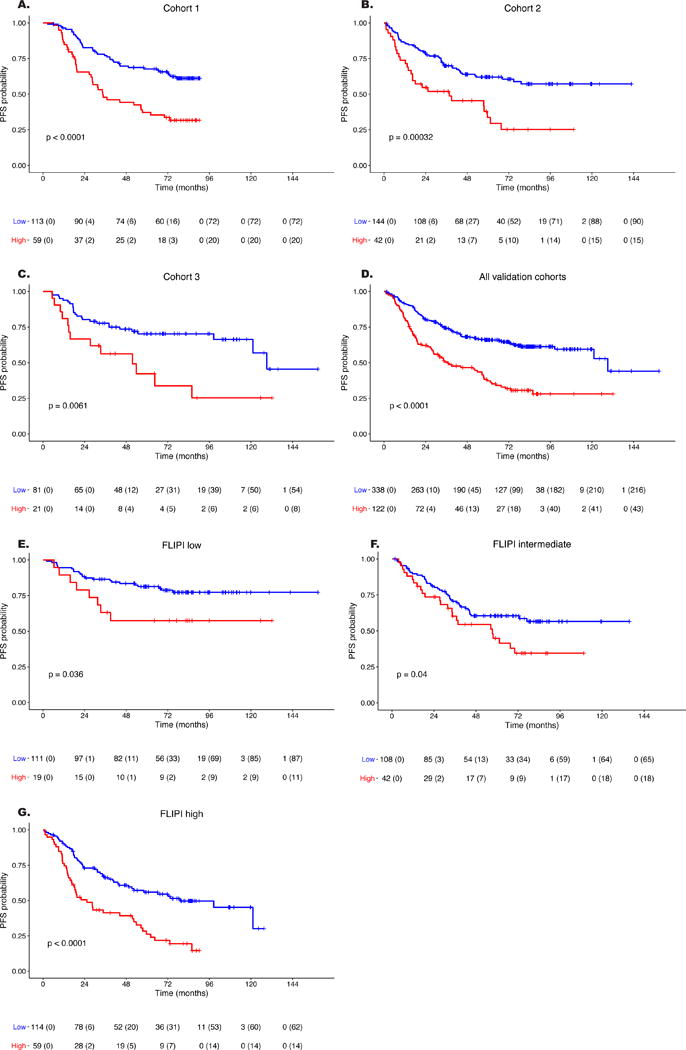
Findings: In the training cohort, the expression levels of 395 genes were associated with a risk of progression. 23 genes reflecting both B-cell biology and tumour microenvironment with correlation coefficients greater than 0·75 between the two technologies and sample types were retained to build a predictive model that identified a population at an increased risk of progression (p<0·0001). In a multivariate Cox model for progression-free survival adjusted on rituximab maintenance treatment and Follicular Lymphoma International Prognostic Index 1 (FLIPI-1) score, this predictor independently predicted progression (adjusted hazard ratio [aHR] of the high-risk group compared with the low-risk group 3·68, 95% CI 2·19-6·17 [p<0·0001]). The 5-year progression-free survival was 26% (95% CI 16-43) in the high-risk group and 73% (64-83) in the low-risk group. The predictor performances were confirmed in each of the individual validation cohorts (aHR comparing high-risk to low-risk groups 2·57 [95% CI 1·65-4·01] in cohort 1; 2·12 [1·32-3·39] in cohort 2; and 2·11 [1·01-4·41] in cohort 3). In the combined validation cohort, the median progression-free survival was 3·1 years (95% CI 2·4-4·8) in the high-risk group and 10·8 years (10·1-not reached) in the low-risk group (p<0·0001). The risk of lymphoma progression at 2 years was 38% (95% CI 29-46) in the high-risk group and 19% (15-24) in the low-risk group. In a multivariate analysis, the score predicted progression-free survival independently of anti-CD20 maintenance treatment and of the FLIPI score (aHR for the combined cohort 2·30, 95% CI 1·72-3·07).
Interpretation: We developed and validated a robust 23-gene expression-based predictor of progression-free survival that is applicable to routinely available formalin-fixed, paraffin-embedded tumour biopsies from patients with follicular lymphoma at time of diagnosis. Applying this score could allow individualised therapy for patients according to their risk category.
Funding: Roche, SIRIC Lyric, LYSARC, National Institutes of Health, the Henry J Predolin Foundation, and the Spanish Plan Nacional de Investigacion.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The other authors declared no conflicts of interest.
Figures
Comment in
-
Predicting early relapse in follicular lymphoma: have we turned a corner?Lancet Oncol. 2018 Apr;19(4):441-442. doi: 10.1016/S1470-2045(18)30114-1. Epub 2018 Feb 20. Lancet Oncol. 2018. PMID: 29475722 No abstract available.
-
Predictive gene-expression score for follicular lymphona.Lancet Oncol. 2018 Jun;19(6):e278. doi: 10.1016/S1470-2045(18)30267-5. Epub 2018 Jun 1. Lancet Oncol. 2018. PMID: 29893253 No abstract available.
-
Predictive gene-expression score for follicular lymphoma.Lancet Oncol. 2018 Jun;19(6):e279. doi: 10.1016/S1470-2045(18)30262-6. Epub 2018 Jun 1. Lancet Oncol. 2018. PMID: 29893254 No abstract available.
-
Predictive gene-expression score for follicular lymphoma.Lancet Oncol. 2018 Jun;19(6):e280. doi: 10.1016/S1470-2045(18)30320-6. Epub 2018 Jun 1. Lancet Oncol. 2018. PMID: 29893255 No abstract available.
-
Predictive gene-expression score for follicular lymphoma.Lancet Oncol. 2018 Jun;19(6):e281. doi: 10.1016/S1470-2045(18)30324-3. Epub 2018 Jun 1. Lancet Oncol. 2018. PMID: 29893256 No abstract available.
-
Predictive gene-expression score for follicular lymphoma - Authors' reply.Lancet Oncol. 2018 Jun;19(6):e282. doi: 10.1016/S1470-2045(18)30339-5. Epub 2018 Jun 1. Lancet Oncol. 2018. PMID: 29893257 No abstract available.
References
-
- Nowakowski GS, Ansell SM. Therapeutic targeting of microenvironment in follicular lymphoma. Hematol Educ Program Am Soc Hematol Am Soc Hematol Educ Program. 2014;2014:169–73. - PubMed
-
- Relander T, Johnson NA, Farinha P, Connors JM, Sehn LH, Gascoyne RD. Prognostic factors in follicular lymphoma. J Clin Oncol Off J Am Soc Clin Oncol. 2010;28:2902–13. - PubMed
-
- Solal-Céligny P, Roy P, Colombat P, et al. Follicular lymphoma international prognostic index. Blood. 2004;104:1258–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
