

Hyperechoic breast images: all that glitters is not gold!
- PMID: 29476429
- PMCID: PMC5893486
- DOI: 10.1007/s13244-017-0590-1
Hyperechoic breast images: all that glitters is not gold!
Abstract
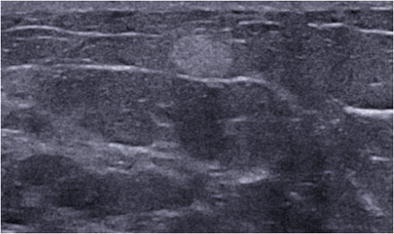
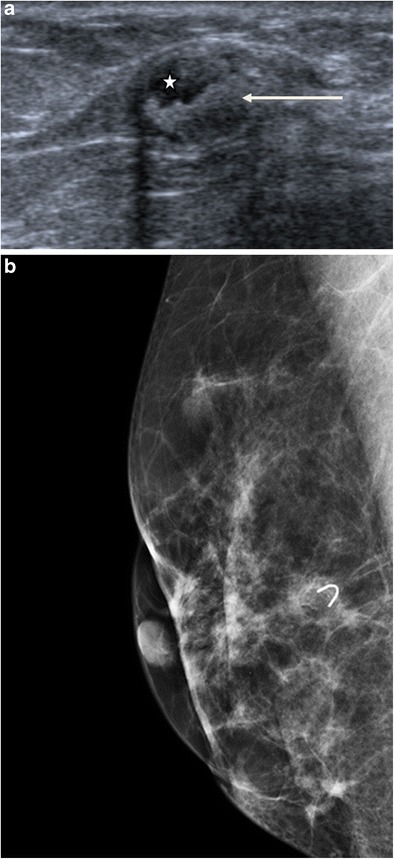
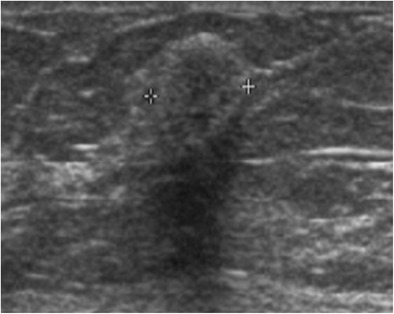
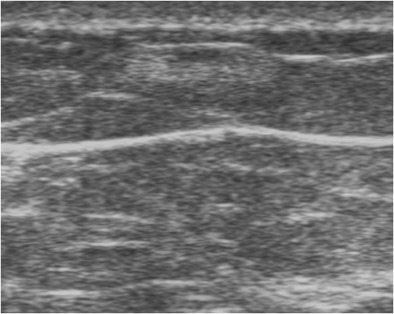
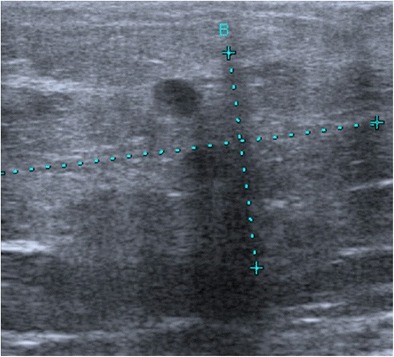
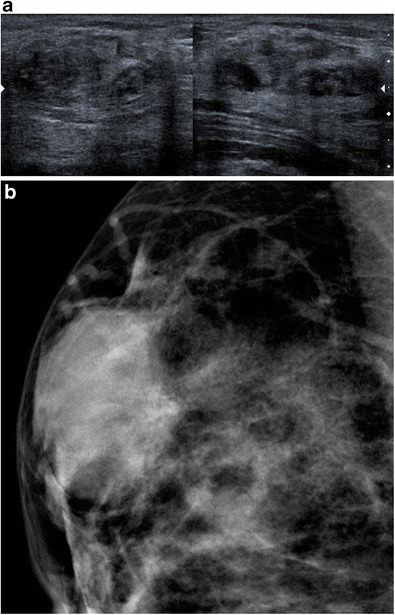
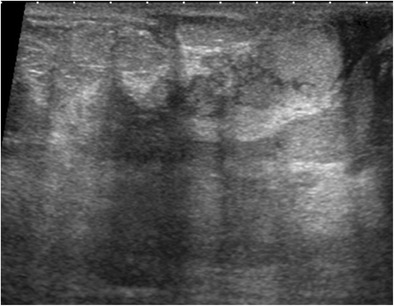
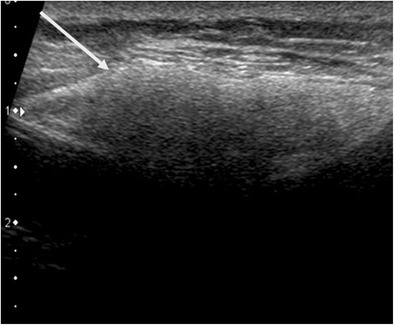
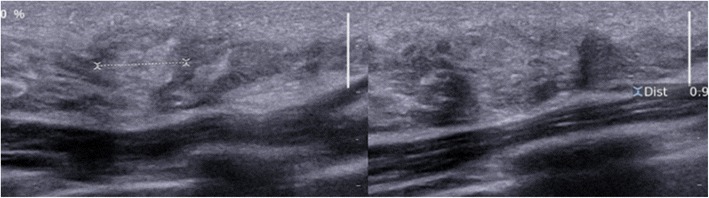
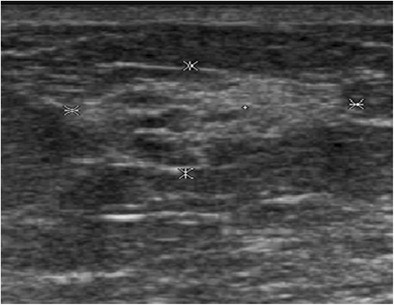
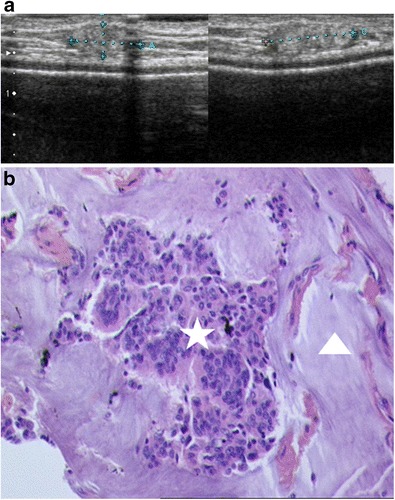
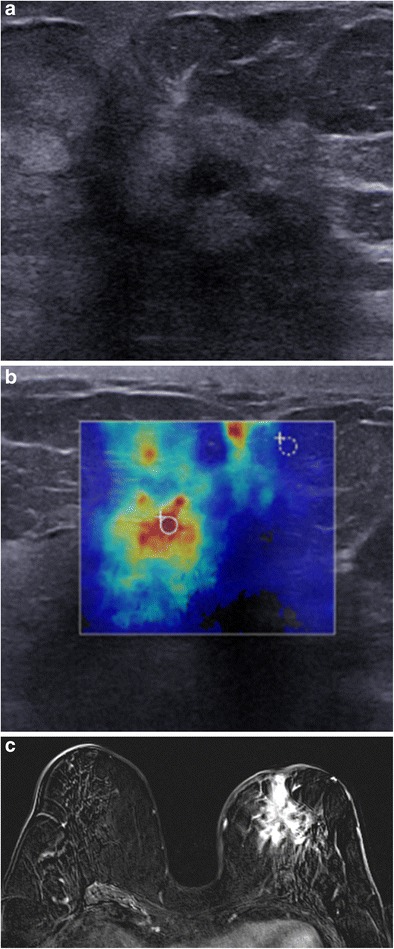
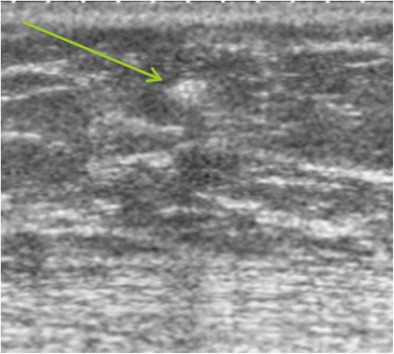
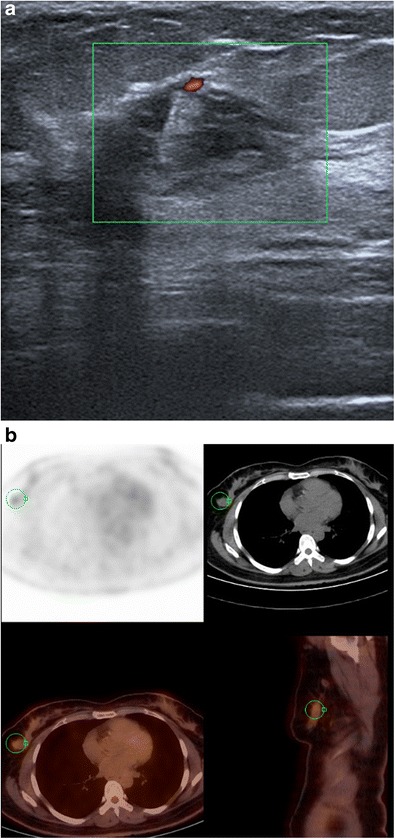
Hyperechogenicity is a sign classically reported to be in favour of a benign lesion and can be observed in many types of benign breast lesions such as hamartoma, lipoma, angiolipoma, haemangioma, haematoma, fat necrosis, fibrosis and galactocele, among others. However, some rare malignant breast lesions can also present a hyperechoic appearance. Most of these hyperechoic malignant lesions present other characteristics that are more typically suggestive of malignancy such as posterior shadowing, a more vertical axis or irregular margins that help to guide the diagnosis. Post magnetic resonance imaging, second-look ultrasound may visualise hyperechoic malignant lesions that would not have been identified at first sight and radiologists must know how to recognise these lesions.
Teaching points: • Some rare malignant breast lesions can present a hyperechoic appearance. • Malignant lesions present other characteristics that are suggestive of malignancy. • An echogenic mass with fat density on mammography does not require biopsy.
Keywords: Breast cancer; Breast ultrasound; Histology; Hyperechogenicity; Malignancy.
Figures





References
-
- American College of Radiology . Illustrated breast imaging reporting and data system (BI-RADS) 3. Reston: American College of Radiology; 1998.
-
- Mendelson EB, Böhm-Vélez M, Berg WA, et al. ACR BI-RADS® ultrasound. In: ACR BI-RADS® atlas, breast imaging reporting and data system. Reston: American College of Radiology; 2013.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
