

Subliminal (latent) processing of pain and its evolution to conscious awareness
- PMID: 29476771
- PMCID: PMC5985199
- DOI: 10.1016/j.neubiorev.2018.02.015
Subliminal (latent) processing of pain and its evolution to conscious awareness
Abstract
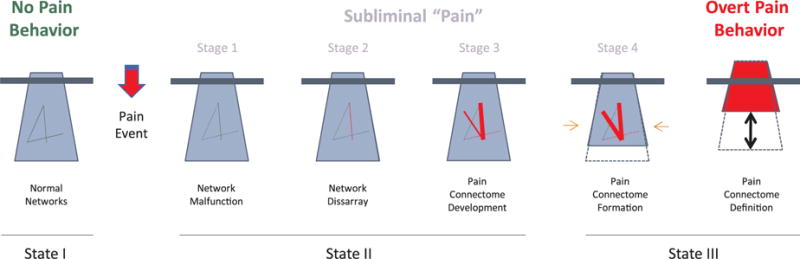
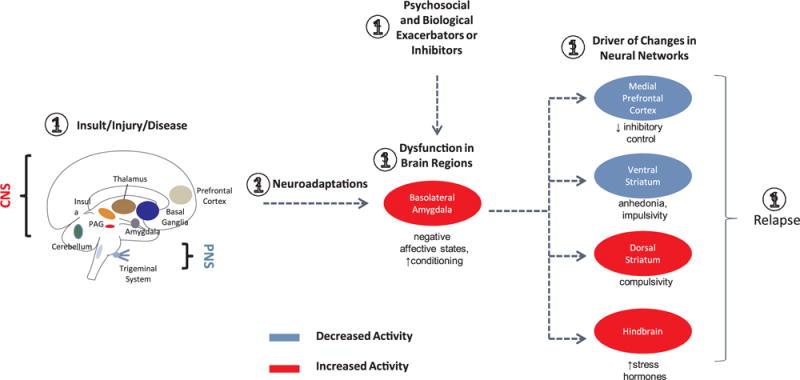
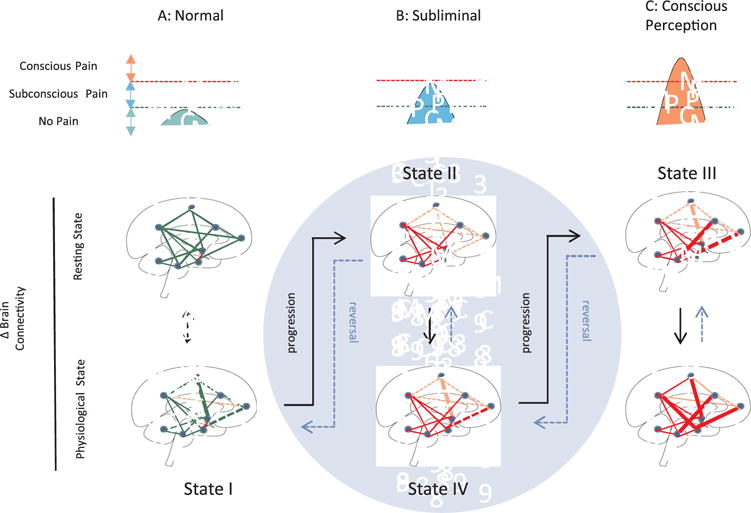
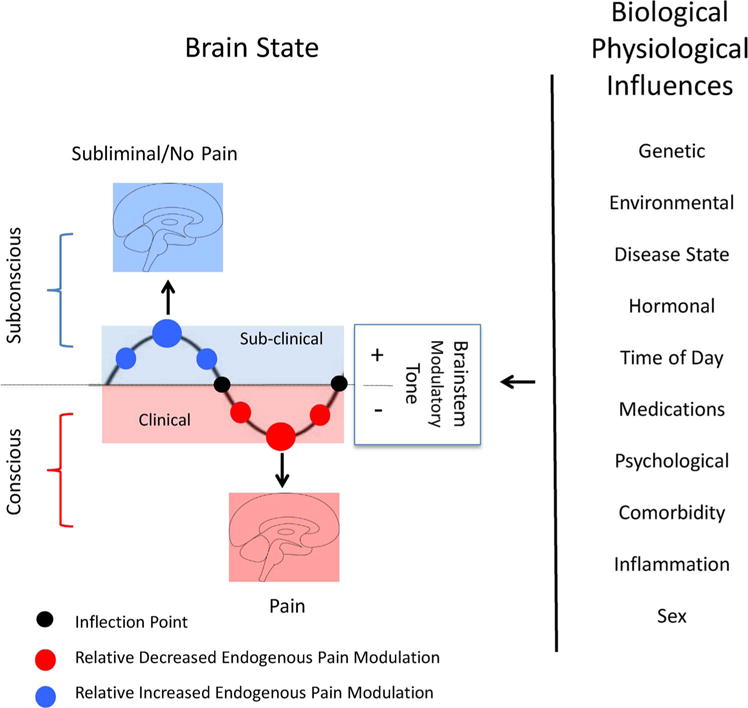
By unconscious or covert processing of pain we refer to nascent interactions that affect the eventual deliverance of pain awareness. Thus, internal processes (viz., repeated nociceptive events, inflammatory kindling, reorganization of brain networks, genetic) or external processes (viz., environment, socioeconomic levels, modulation of epigenetic status) contribute to enhancing or inhibiting the presentation of pain awareness. Here we put forward the notion that for many patients, ongoing sub-conscious changes in brain function are significant players in the eventual manifestation of chronic pain. In this review, we provide clinical examples of nascent or what we term pre-pain processes and the neurobiological mechanisms of how these changes may contribute to pain, but also potential opportunities to define the process for early therapeutic interventions.
Keywords: Awareness; Brain; Chronic pain; Cognition; Iceberg; Neural networks; Subconscious.
Copyright © 2018. Published by Elsevier Ltd.
Conflict of interest statement
None.
Figures
References
-
- Abdallah CG, Geha P. Chronic pain and chronic stress: two sides of the Same coin? Chronic Stress (Thousand Oaks) 2017 http://dx.doi.org/10.1177/2470547017704763. - DOI - PMC - PubMed
-
- Ackerman WE, 3rd, Ahmad M. Recurrent postoperative CRPS I in patients with abnormal preoperative sympathetic function. J Hand Surg Am. 2008;33:217–222. - PubMed
-
- Anand P, Birch R. Restoration of sensory function and lack of long-term chronic pain syndromes after brachial plexus injury in human neonates. Brain. 2002;125:113–122. - PubMed
-
- Andersen KG, Duriaud HM, Jensen HE, Kroman N, Kehlet H. Predictive factors for the development of persistent pain after breast cancer surgery. Pain. 2015;156:2413–2422. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
