

Long-term visit-to-visit glycemic variability as predictor of micro- and macrovascular complications in patients with type 2 diabetes: The Rio de Janeiro Type 2 Diabetes Cohort Study
- PMID: 29477146
- PMCID: PMC6389075
- DOI: 10.1186/s12933-018-0677-0
Long-term visit-to-visit glycemic variability as predictor of micro- and macrovascular complications in patients with type 2 diabetes: The Rio de Janeiro Type 2 Diabetes Cohort Study
Abstract
Background: Long-term visit-to-visit glycemic variability is an additional measure of glycemic control. We aimed to evaluate the prognostic value of several measures of glycemic variability for the occurrence of micro- and macrovascular complications, and all-cause mortality in patients with type 2 diabetes.
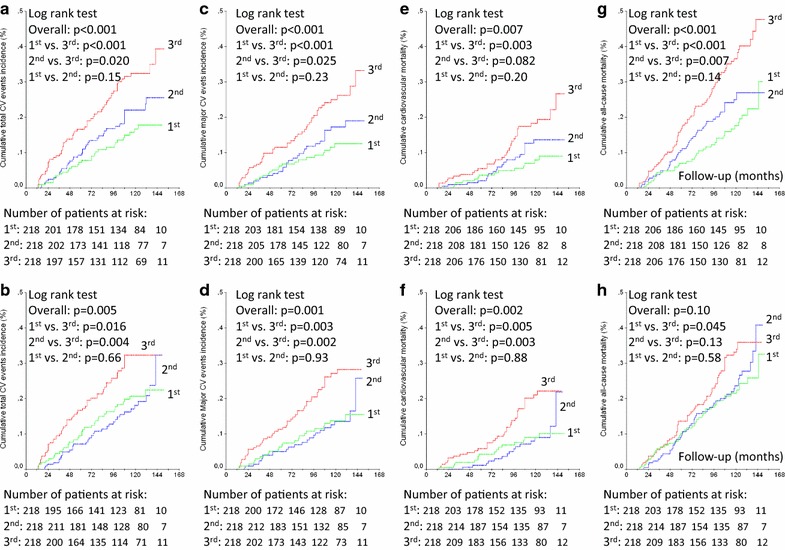
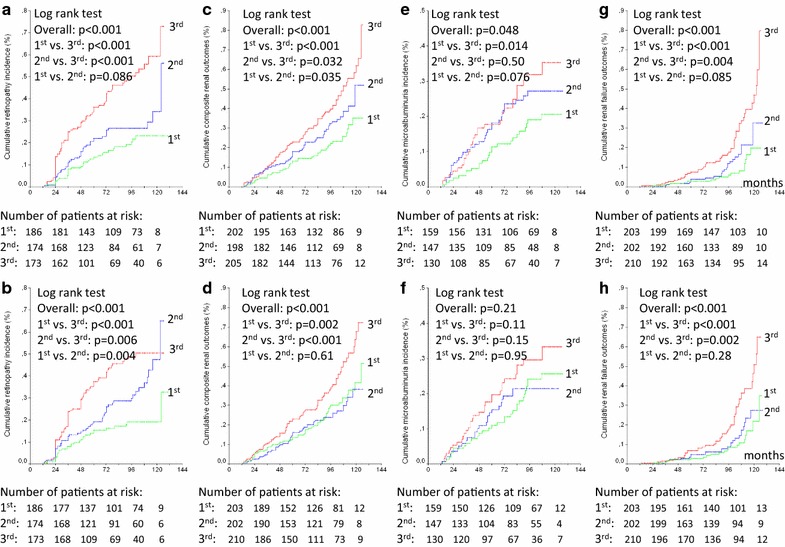
Methods: 654 individuals were followed-up over a median of 9.3 years. Glycemic variability (SDs and coefficients of variation of HbA1c and fasting glycaemia) was measured during the first 12- and 24-months. Multivariate Cox analysis, adjusted for risk factors and mean HbA1c and fasting glycaemia levels, examined the associations between glycemic variability and the occurrence of microvascular (retinopathy, microalbuminuria, renal function deterioration, peripheral neuropathy) and macrovascular complications [total cardiovascular events (CVE), major adverse CVEs (MACE) and cardiovascular mortality], and of all-cause mortality.
Results: During follow-up, 128 patients had a CVE (96 MACE), and 158 patients died (67 from cardiovascular diseases); 152 newly-developed or worsened diabetic retinopathy, 183 achieved the renal composite outcome (89 newly developed microalbuminuria and 91 deteriorated renal function), and 96 newly-developed or worsened peripheral neuropathy. Glycemic variability, particularly the 24-month parameters either estimated by HbA1c or by fasting glycemia, predicted all endpoints, except for retinopathy and peripheral neuropathy development/progression, and was a better predictor than mean HbA1c. Glycemic variability predicted retinopathy development/progression in patients with good glycemic control (HbA1c ≤ 7.5%, 58 mmol/mol) and predicted new-incident peripheral neuropathy.
Conclusions: Long-term visit-to-visit glycemic variability is an additional and frequently a better glycemic parameter than mean HbA1c levels for assessing the risk of future development of micro- and macrovascular complications in patients with type 2 diabetes.
Keywords: Glycemic variability; Macrovascular complications; Microvascular complications; Mortality; Type 2 diabetes.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
