

Activation of AQP2 water channels without vasopressin: therapeutic strategies for congenital nephrogenic diabetes insipidus
- PMID: 29478202
- PMCID: PMC5956045
- DOI: 10.1007/s10157-018-1544-8
Activation of AQP2 water channels without vasopressin: therapeutic strategies for congenital nephrogenic diabetes insipidus
Abstract
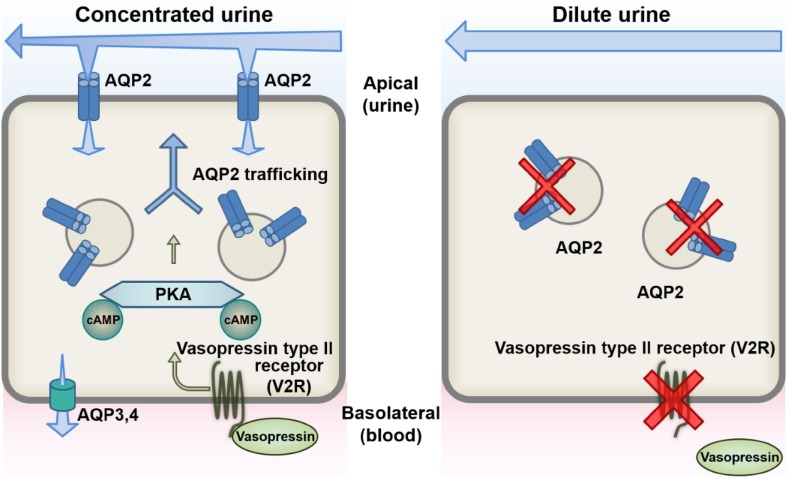
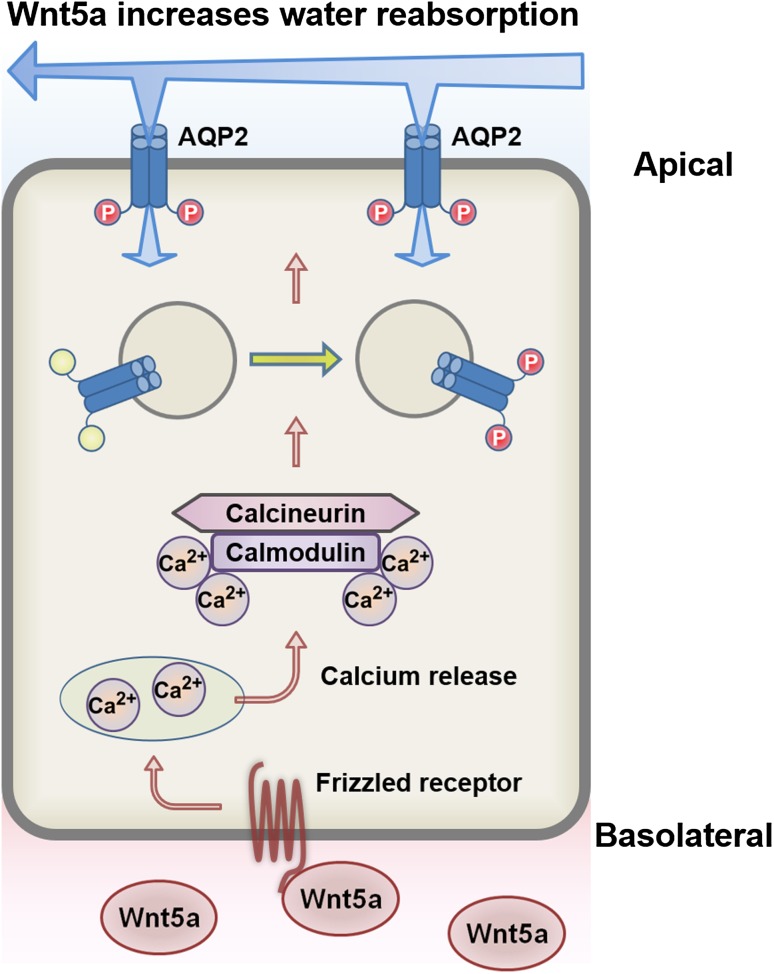
Congenital nephrogenic diabetes insipidus (NDI) is characterized by defective urine concentrating ability. Symptomatic polyuria is present from birth, even with normal release of the antidiuretic hormone vasopressin by the pituitary. Over the last two decades, the aquaporin-2 (AQP2) gene has been cloned and the molecular mechanisms of urine concentration have been gradually elucidated. Vasopressin binds to the vasopressin type II receptor (V2R) in the renal collecting ducts and then activates AQP2 phosphorylation and trafficking to increase water reabsorption from urine. Most cases of congenital NDI are caused by loss-of-function mutations to V2R, resulting in unresponsiveness to vasopressin. In this article, we provide an overview of novel therapeutic molecules of congenital NDI that can activate AQP2 by bypassing defective V2R signaling with a particular focus on the activators of the calcium and cAMP signaling pathways.
Keywords: AQP2; Calcium signaling; Congenital nephrogenic diabetes insipidus; GPCRs agonists; PDE inhibitors; cAMP signaling.
Conflict of interest statement
Conflict of interest
The authors have declared that no conflict of interest exists.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
