

Potential Adverse Effects of Broad-Spectrum Antimicrobial Exposure in the Intensive Care Unit
- PMID: 29479546
- PMCID: PMC5804637
- DOI: 10.1093/ofid/ofx270
Potential Adverse Effects of Broad-Spectrum Antimicrobial Exposure in the Intensive Care Unit
Abstract
Background: The potential adverse effects of empiric broad-spectrum antimicrobial use among patients with suspected but subsequently excluded infection have not been fully characterized. We sought novel methods to quantify the risk of adverse effects of broad-spectrum antimicrobial exposure among patients admitted to an intensive care unit (ICU).
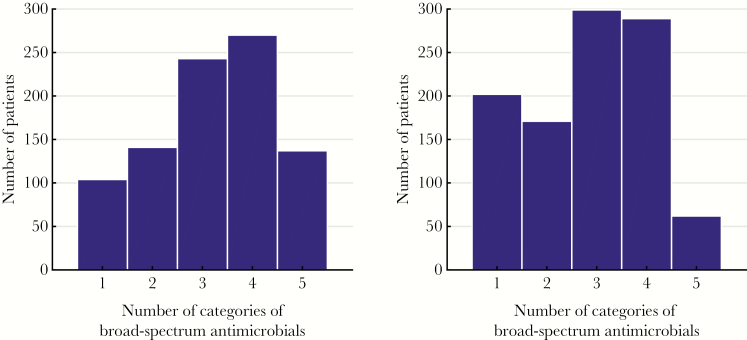
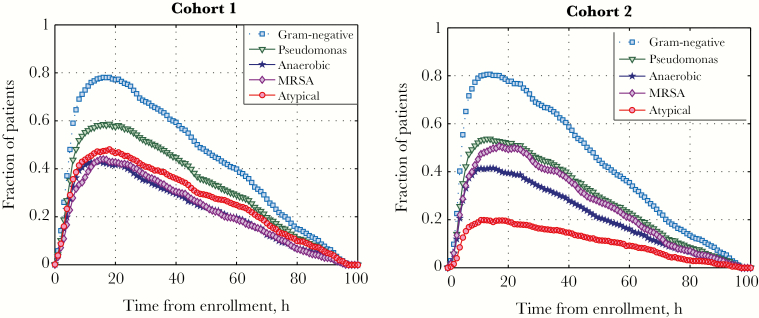
Methods: Among all adult patients admitted to ICUs at a single institution, we selected patients with negative blood cultures who also received ≥1 broad-spectrum antimicrobials. Broad-spectrum antimicrobials were categorized in ≥1 of 5 categories based on their spectrum of activity against potential pathogens. We performed, in serial, 5 cohort studies to measure the effect of each broad-spectrum category on patient outcomes. Exposed patients were defined as those receiving a specific category of broad-spectrum antimicrobial; nonexposed were all other patients in the cohort. The primary outcome was 30-day mortality. Secondary outcomes included length of hospital and ICU stay and nosocomial acquisition of antimicrobial-resistant bacteria (ARB) or Clostridium difficile within 30 days of admission.
Results: Among the study cohort of 1918 patients, 316 (16.5%) died within 30 days, 821 (42.8%) had either a length of hospital stay >7 days or an ICU length of stay >3 days, and 106 (5.5%) acquired either a nosocomial ARB or C. difficile. The short-term use of broad-spectrum antimicrobials in any of the defined broad-spectrum categories was not significantly associated with either primary or secondary outcomes.
Conclusions: The prompt and brief empiric use of defined categories of broad-spectrum antimicrobials could not be associated with additional patient harm.
Keywords: antibiotic stewardship; antimicrobials; broad-spectrum; intensive care unit; nosocomial.
Figures
References
-
- Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients. Chest 1999; 115:462–74. - PubMed
-
- Harbarth S, Garbino J, Pugin J et al. . Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med 2003; 115:529–35. - PubMed
-
- American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005; 171:388–416. - PubMed
-
- Kumar A, Ellis P, Arabi Y et al. ; Cooperative Antimicrobial Therapy of Septic Shock Database Research Group Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest 2009; 136:1237–48. - PubMed
-
- Kumar A, Safdar N, Kethireddy S, Chateau D. A survival benefit of combination antibiotic therapy for serious infections associated with sepsis and septic shock is contingent only on the risk of death: a meta-analytic/meta-regression study. Crit Care Med 2010; 38:1651–64. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
