

Anatomical and Radiological Considerations When Colonic Perforation Leads to Subcutaneous Emphysema, Pneumothoraces, Pneumomediastinum, and Mediastinal Shift
- PMID: 29479562
- PMCID: PMC5823697
- DOI: 10.1055/s-0038-1624563
Anatomical and Radiological Considerations When Colonic Perforation Leads to Subcutaneous Emphysema, Pneumothoraces, Pneumomediastinum, and Mediastinal Shift
Abstract
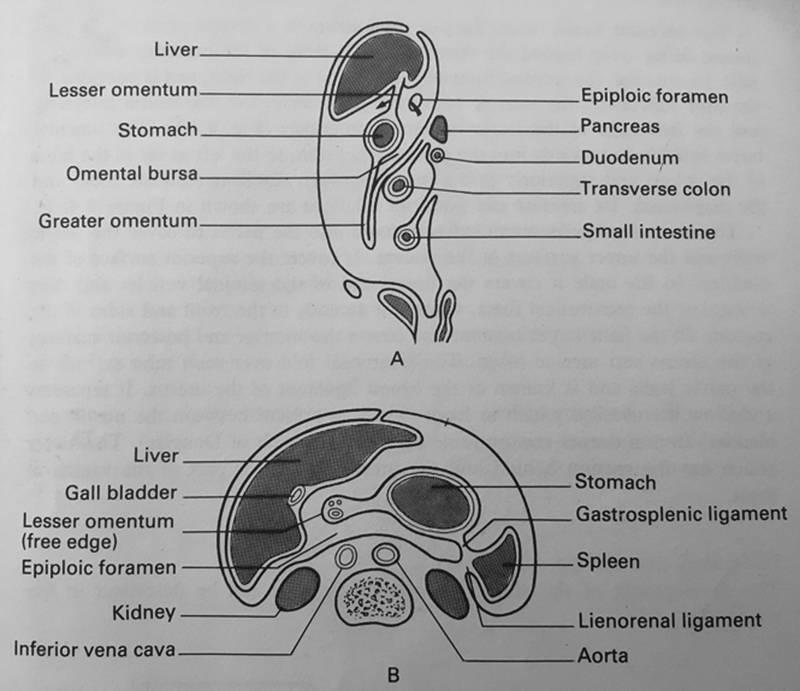
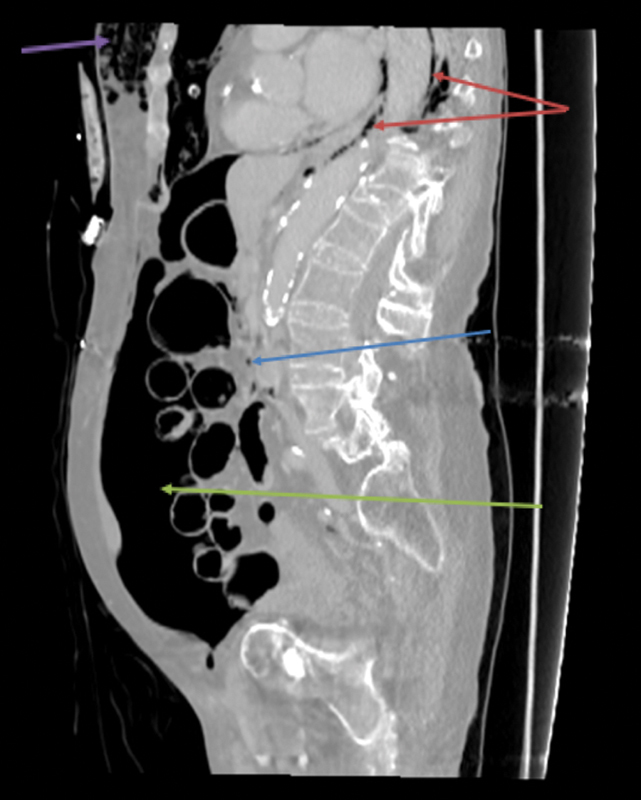
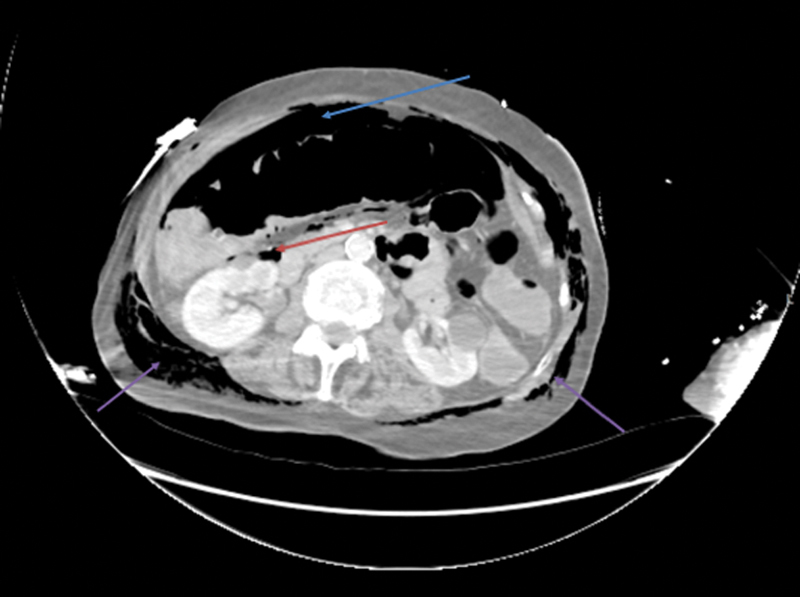
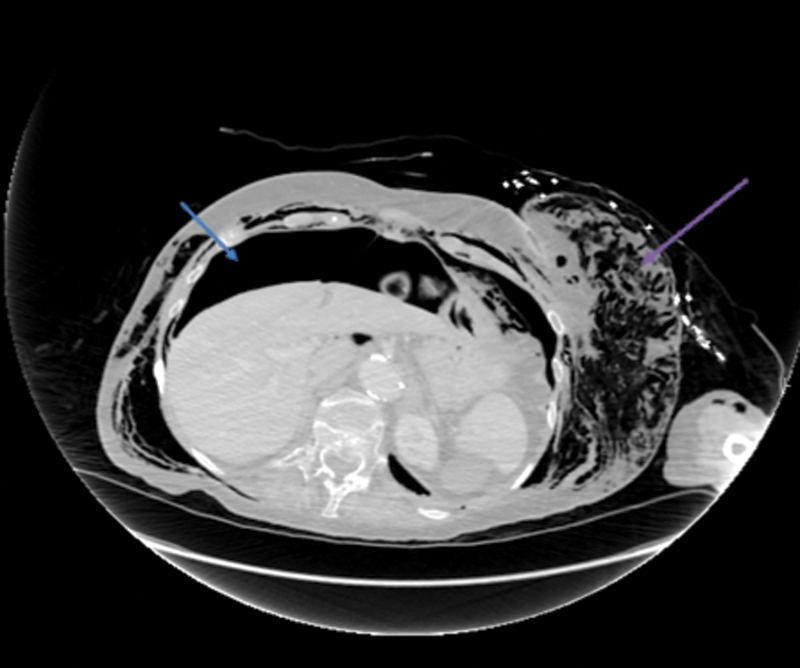
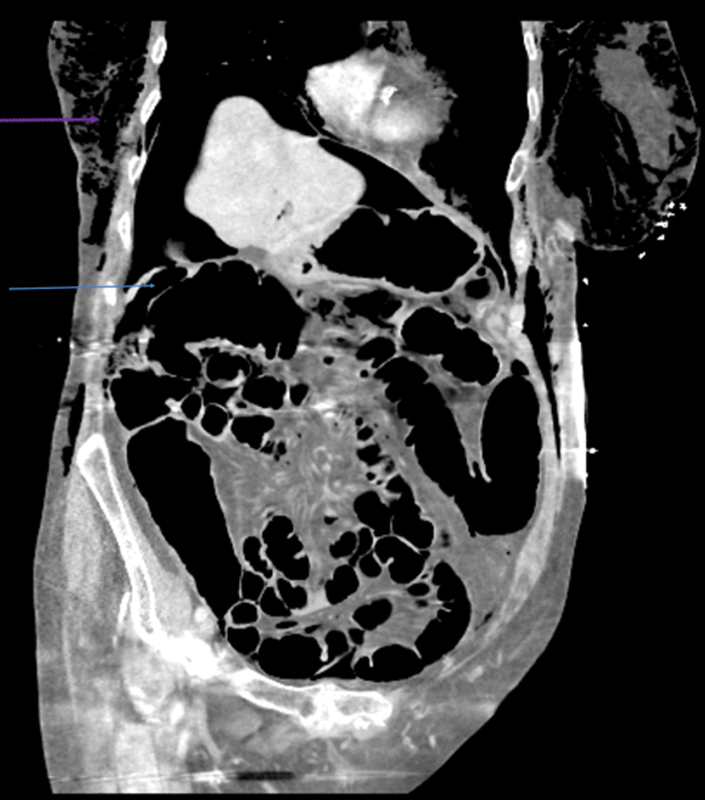
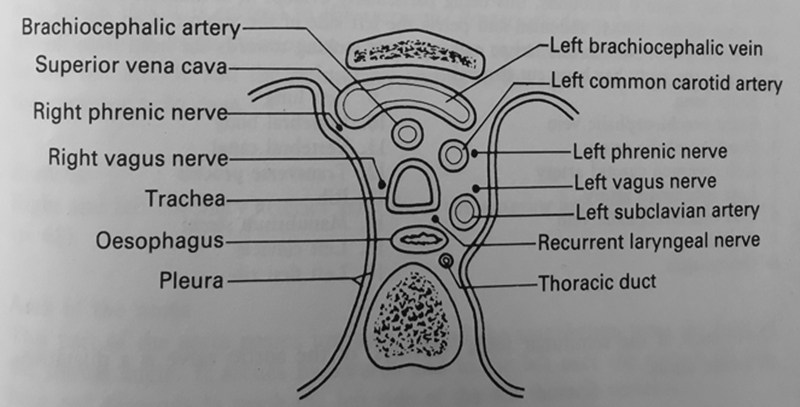
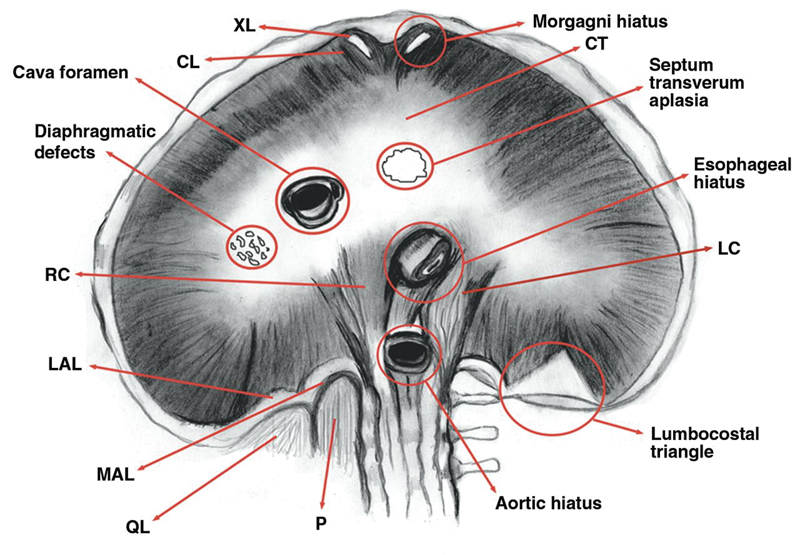
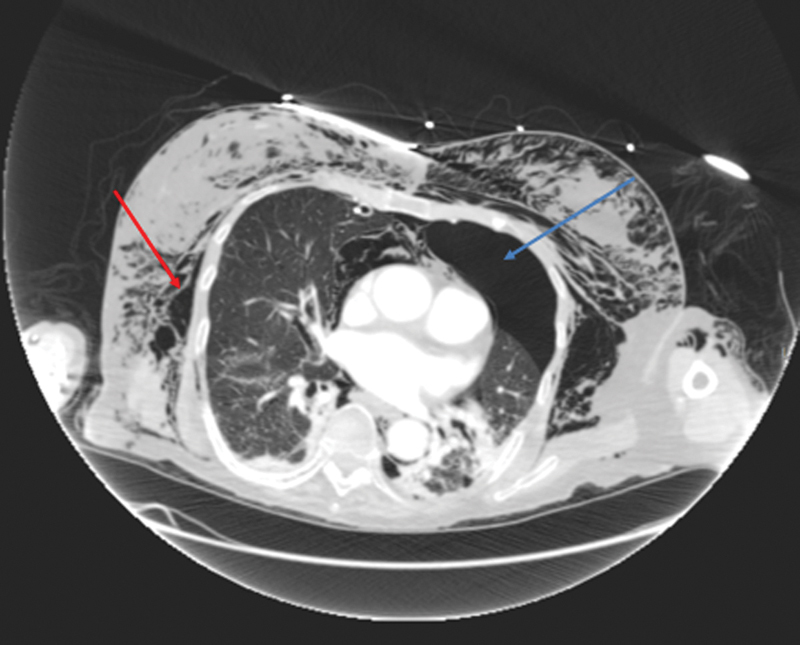
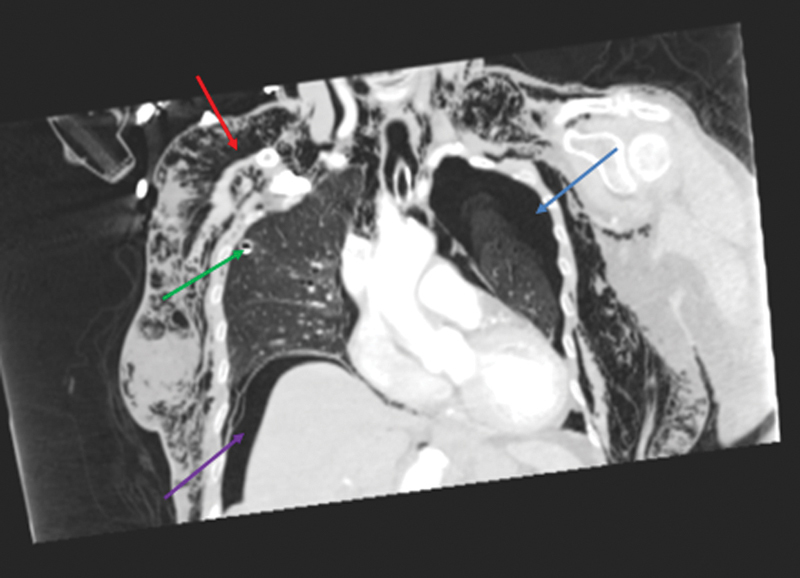
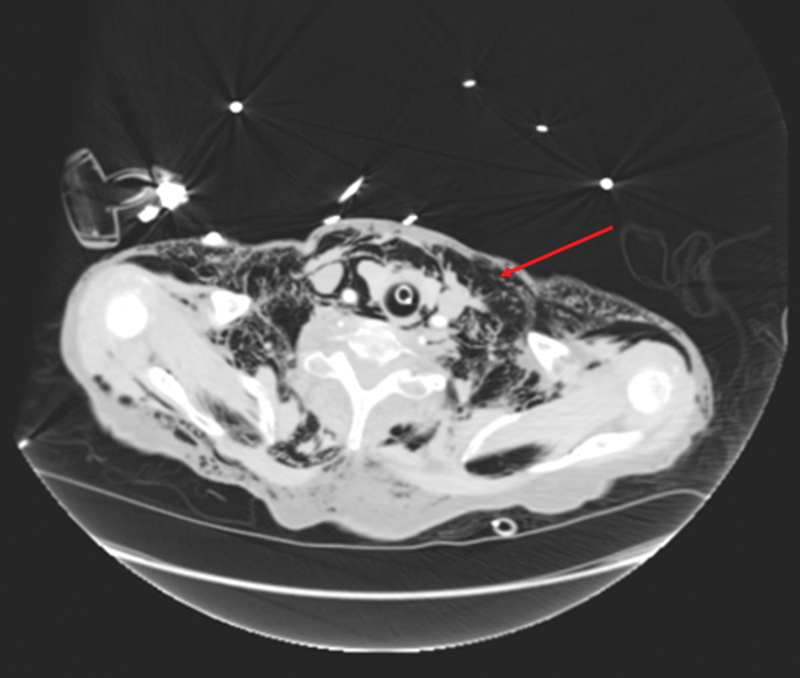
While colonoscopy is generally regarded as a safe procedure, colonic perforation can occur and the risk of this is higher when interventional procedures are undertaken. The presentation may be acute or delayed depending on the extent of the perforation. Extracolonic gas following colonic perforation can migrate to several body compartments that are embryologically related and it has previously been reported in the thorax, mediastinum, neck, scrotum, and lower limbs. This review discusses in detail the anatomical pathways that led to a rare case of widespread subcutaneous emphysema, bilateral pneumothoraces, pneumomediastinum, and mediastinal shift from colonic perforation during a diagnostic colonoscopy. This is further supported by a description of the radiological images.
Keywords: anatomical; colonoscopy; perforation; pneumomediastinum; pneumothorax; radiology.
Conflict of interest statement
Figures
Similar articles
-
Pneumoretroperitoneum, Pneumomediastinum, Pneumothorax, and Subcutaneous Emphysema after Diagnostic Colonoscopy.Korean J Gastroenterol. 2017 Sep 25;70(3):145-149. doi: 10.4166/kjg.2017.70.3.145. Korean J Gastroenterol. 2017. PMID: 28934831
-
Mediastinal, retroperitoneal, and subcutaneous emphysema due to sigmoid colon penetration: A case report and literature review.Int J Surg Case Rep. 2019;55:213-217. doi: 10.1016/j.ijscr.2019.02.003. Epub 2019 Feb 10. Int J Surg Case Rep. 2019. PMID: 30771625 Free PMC article.
-
Pneumomediastinum, Pneumothorax, and Subcutaneous Emphysema Caused by Colonoscopic Perforation: A Report of Two Cases.J Emerg Med. 2017 Apr;52(4):e117-e122. doi: 10.1016/j.jemermed.2016.10.047. Epub 2016 Nov 19. J Emerg Med. 2017. PMID: 27876330
-
Head and neck subcutaneous emphysema, a rare complication of iatrogenic perforation during colonoscopy: management review of reported cases from 2000-2016.Expert Rev Gastroenterol Hepatol. 2017 Sep;11(9):849-856. doi: 10.1080/17474124.2017.1351294. Epub 2017 Jul 19. Expert Rev Gastroenterol Hepatol. 2017. PMID: 28678570 Review.
-
Bilateral spontaneous pneumothoraces, pneumopericardium, pneumomediastinum, and subcutaneous emphysema: a rare presentation of paraquat intoxication.Ann Emerg Med. 1994 May;23(5):1132-4. doi: 10.1016/s0196-0644(94)70116-4. Ann Emerg Med. 1994. PMID: 8185113 Review.
Cited by
-
Self-Inflicted Abdominal Air Insufflation Leading to Diffuse Subcutaneous Emphysema, Pneumoperitoneum, Pneumomediastinum, Pneumopericardium, and Pneumothorax: A Case Report.Cureus. 2022 Oct 13;14(10):e30278. doi: 10.7759/cureus.30278. eCollection 2022 Oct. Cureus. 2022. PMID: 36381859 Free PMC article.
-
Pneumomediastinum, Pneumoretroperitoneum, Pneumoperitoneum and Subcutaneous Emphysema Secondary to a Penetrating Anal Injury.Diagnostics (Basel). 2021 Apr 15;11(4):707. doi: 10.3390/diagnostics11040707. Diagnostics (Basel). 2021. PMID: 33920850 Free PMC article.
-
Bilateral pneumothorax and pneumomediastinum during colonoscopy in a patient with intestinal Behcet's disease: A case report.World J Clin Cases. 2022 Feb 26;10(6):2030-2035. doi: 10.12998/wjcc.v10.i6.2030. World J Clin Cases. 2022. PMID: 35317145 Free PMC article.
-
Pneumothorax, Pneumomediastinum, and Cervical and Facial Massive Emphysema Secondary to Colonoscopy: A Rare Complication of Colonoscopy.Case Rep Gastrointest Med. 2024 Jun 25;2024:1140099. doi: 10.1155/2024/1140099. eCollection 2024. Case Rep Gastrointest Med. 2024. PMID: 38957575 Free PMC article.
-
Acute subcutaneous emphysema: A rare clinical presentation of large bowel perforation.JRSM Open. 2023 Feb 8;14(2):20542704231153529. doi: 10.1177/20542704231153529. eCollection 2023 Feb. JRSM Open. 2023. Retraction in: JRSM Open. 2024 Jun 6;15(6):20542704241260533. doi: 10.1177/20542704241260533. PMID: 36776619 Free PMC article. Retracted.
References
-
- The NHS Atlas of variation.Rate of colonoscopy procedures and flexisigmoidoscopy procedures per population per PCT2011 Atlas_2011_CancerMaps.pdf.https://fingertips.phe.org.uk/documents/atlas_2011_CancerMaps.pdf. Accessed February 15, 2018
-
- Waye J D. Colonoscopy. CA Cancer J Clin. 1992;42(06):350–365. - PubMed
-
- Ho H C, Burchell S, Morris P, Yu M. Colon perforation, bilateral pneumothoraces, pneumopericardium, pneumomediastinum, and subcutaneous emphysema complicating endoscopic polypectomy: anatomic and management considerations. Am Surg. 1996;62(09):770–774. - PubMed
-
- Ignjatović M, Jović J. Tension pneumothorax, pneumoretroperitoneum, and subcutaneous emphysema after colonoscopic polypectomy: a case report and review of the literature. Langenbecks Arch Surg. 2009;394(01):185–189. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources