

Variation among cleft centres in the use of secondary surgery for children with cleft palate: a retrospective cohort study
- PMID: 29479567
- PMCID: PMC5823530
- DOI: 10.1136/bmjpo-2017-000063
Variation among cleft centres in the use of secondary surgery for children with cleft palate: a retrospective cohort study
Abstract
Objectives: To test whether cleft centres vary in their use of secondary cleft palate surgery, also known as revision palate surgery, and if so to identify modifiable hospital- and surgeon-factors that are associated with use of secondary surgery.
Design: Retrospective cohort study.
Setting: Forty-three paediatric hospitals across the United States.
Patients: Children with cleft lip and palate who underwent primary cleft palate repair from 1999 to 2013.
Main outcome measures: Time from primary cleft palate repair to secondary palate surgery.
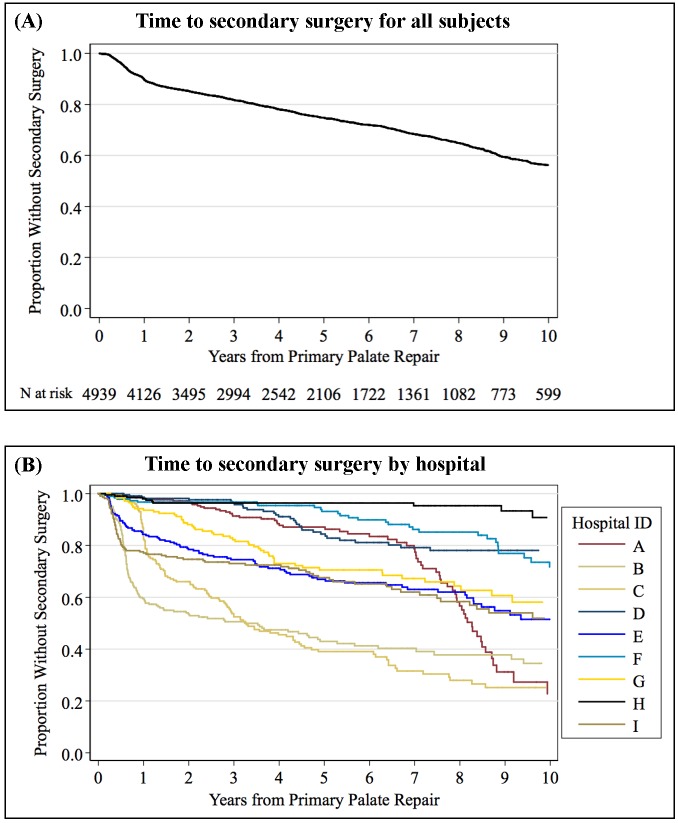
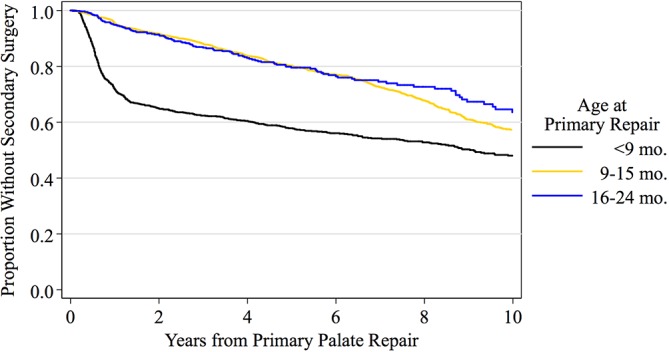
Results: We identified 4,939 children who underwent primary cleft palate repair. At ten years after primary palate repair, 44% of children had undergone secondary palate surgery. Significant variation existed among hospitals (p<0.001); the proportion of children undergoing secondary surgery by 10 years ranged from 9% to 77% across hospitals. After adjusting for patient demographics, primary palate repair before nine months of age was associated with an increased hazard of secondary palate surgery (initial hazard ratio 6.74, 95% CI 5.30-8.73). Postoperative antibiotics, surgeon procedure volume, and hospital procedure volume were not associated with time to secondary surgery (p>0.05). Of the outcome variation attributable to hospitals and surgeons, between-hospital differences accounted for 59% (p<0.001), while between-surgeon differences accounted for 41% (p<0.001).
Conclusions: Substantial variation in the hazard of secondary palate surgery exists depending on a child's age at primary palate repair and the hospital and surgeon performing their repair. Performing primary palate repair before nine months of age substantially increases the hazard of secondary surgery. Further research is needed to identify other factors contributing to variation in palate surgery outcomes among hospitals and surgeons.
Keywords: Health Services Research; Outcomes Research; Plastic Surgery; Procedures.
Conflict of interest statement
COMPETING INTERESTS All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; Dr. Britto reports personal fees and other from American Board of Pediatrics Research Advisory Committee, outside the submitted work; all other authors report no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Five-Fold Variation Among Surgeons and Hospitals in the Use of Secondary Palate Surgery.Cleft Palate Craniofac J. 2019 May;56(5):586-594. doi: 10.1177/1055665618799906. Epub 2018 Sep 24. Cleft Palate Craniofac J. 2019. PMID: 30244603 Free PMC article.
-
Marked Variation Exists Among Surgeons and Hospitals in the Use of Secondary Cleft Lip Surgery.Cleft Palate Craniofac J. 2020 Feb;57(2):198-207. doi: 10.1177/1055665619880056. Epub 2019 Oct 9. Cleft Palate Craniofac J. 2020. PMID: 31597471 Free PMC article.
-
Is Risk of Secondary Surgery for Oronasal Fistula Following Primary Cleft Palate Repair Associated With Hospital Case Volume and Cost-to-Charge Ratio?Cleft Palate Craniofac J. 2021 May;58(5):603-611. doi: 10.1177/1055665620959528. Cleft Palate Craniofac J. 2021. PMID: 33840261
-
Does the type of cleft palate contribute to the need for secondary surgery? A national perspective.Laryngoscope. 2013 Oct;123(10):2387-91. doi: 10.1002/lary.24008. Epub 2013 Aug 5. Laryngoscope. 2013. PMID: 23918465
-
Cleft Lip and Cleft Palate Surgery: Malpractice Litigation Outcomes.Cleft Palate Craniofac J. 2017 Jan;54(1):75-79. doi: 10.1597/15-285. Epub 2016 Feb 16. Cleft Palate Craniofac J. 2017. PMID: 26882025 Review.
Cited by
-
Non-Interventional Factors Influencing Velopharyngeal Function For Speech In Initial Cleft Palate Repair: A Systematic Review Protocol.Syst Rev. 2019 Nov 5;8(1):261. doi: 10.1186/s13643-019-1141-2. Syst Rev. 2019. PMID: 31690349 Free PMC article.
-
Five-Fold Variation Among Surgeons and Hospitals in the Use of Secondary Palate Surgery.Cleft Palate Craniofac J. 2019 May;56(5):586-594. doi: 10.1177/1055665618799906. Epub 2018 Sep 24. Cleft Palate Craniofac J. 2019. PMID: 30244603 Free PMC article.
-
Analysis and Reporting of Randomized Trials in Cleft Palate Surgery: Learning from the Timing of Primary Surgery (TOPS) Trial.Cleft Palate Craniofac J. 2025 Aug;62(8):1436-1442. doi: 10.1177/10556656241253949. Epub 2024 May 9. Cleft Palate Craniofac J. 2025. PMID: 38725271 Free PMC article.
References
-
- Parker SE, Mai CT, Canfield MA, et al. . Updated National Birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol 2010;88:1008–16. doi:10.1002/bdra.20735 - DOI - PubMed
-
- Watkins SE, Meyer RE, Strauss RP, et al. . Classification, epidemiology, and genetics of orofacial clefts. Clin Plast Surg 2014;41:149–63. doi:10.1016/j.cps.2013.12.003 - DOI - PubMed
-
- IPDTOC Working Group. Prevalence at birth of cleft lip with or without cleft palate: data from the International Perinatal database of typical oral clefts (IPDTOC). Cleft Palate Craniofac J 2011;48:66–81. doi:10.1597/09-217 - DOI - PubMed
-
- Smith DM, Losee JE. Cleft palate repair. Clin Plast Surg 2014;41:189–210. doi:10.1016/j.cps.2013.12.005 - DOI - PubMed
-
- Allareddy V, Turkistani K, Nanda V, et al. . Factors associated with hospitalization charges for cleft palate repairs and revisions. J Oral Maxillofac Surg 2012;70:1968–77. doi:10.1016/j.joms.2011.07.026 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources