

Spectral domain optical coherence tomography evaluation of macular changes in Eales disease
- PMID: 29480258
- PMCID: PMC5859602
- DOI: 10.4103/ijo.IJO_845_17
Spectral domain optical coherence tomography evaluation of macular changes in Eales disease
Abstract
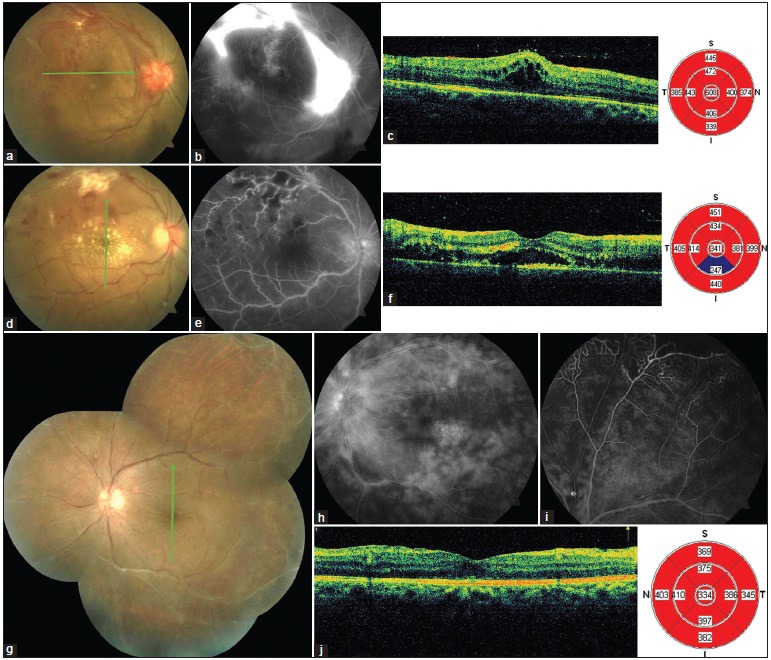
Purpose: The purpose of the study was to describe macular changes in treatment-naïve eyes with Eales disease using spectral domain optical coherence tomography (SD-OCT).
Methods: A cross-sectional study was done on 79 eyes of 66 patients with Eales disease. Best-corrected visual acuity (BCVA), slit-lamp biomicroscopy (SLB), indirect ophthalmoscopy, fundus fluorescein angiography (FFA), and quantitative (central macular thickness [CMT]) and qualitative analysis on SD-OCT were performed.
Results: Forty-six (58.2%) eyes had macular involvement as assessed with SD-OCT, while in 33 (41.8%) eyes, macula was not affected. Macular edema was the most common feature when macula was affected followed by epiretinal membrane. Mean CMT was higher (315.3 ± 102.3 μm) in eyes with macular involvement than those without it (243.8 ± 19.3 μm). Eyes with active vasculitis involving larger vessels and neovascularization had greater chance of macular involvement. SLB and FFA alone missed 28.3% and 50% eyes with macular abnormalities on SD-OCT, respectively.
Conclusion: While the clinical description of Eales disease points mainly to a peripheral location, macular involvement can be commonly picked up when SD-OCT is used. Macular involvement when present is associated with a poorer BCVA.
Keywords: Eales disease; epiretinal membrane; macula; macular edema; retinal vasculitis; spectral domain optical coherence tomography.
Conflict of interest statement
There are no conflicts of interest.
Figures




Comment in
-
Macular changes in retinal vasculitis.Indian J Ophthalmol. 2018 Mar;66(3):439. doi: 10.4103/ijo.IJO_1232_17. Indian J Ophthalmol. 2018. PMID: 29480259 Free PMC article. No abstract available.
References
-
- Das T, Pathengay A, Hussain N, Biswas J. Eales’ disease: Diagnosis and management. Eye (Lond) 2010;24:472–82. - PubMed
-
- Biswas J, Sharma T, Gopal L, Madhavan HN, Sulochana KN, Ramakrishnan S, et al. Eales disease – An update. Surv Ophthalmol. 2002;47:197–214. - PubMed
-
- Badrinath SS, Honnatti MR. Vitrectomy in Eales disease. Acta Int Cong Ophthalmol. 1982;24:536.
-
- Saxena S, Kumar D. New classification system-based visual outcome in Eales’ disease. Indian J Ophthalmol. 2007;55:267–9. - PubMed
-
- Saxena S, Kumar D. Macular involvement in Eales disease. Ann Ophthalmol. 2000;32:98–100.
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
