

Meta-analysis of risk of developing malignancy in congenital choledochal malformation
- PMID: 29480528
- PMCID: PMC5900735
- DOI: 10.1002/bjs.10798
Meta-analysis of risk of developing malignancy in congenital choledochal malformation
Abstract
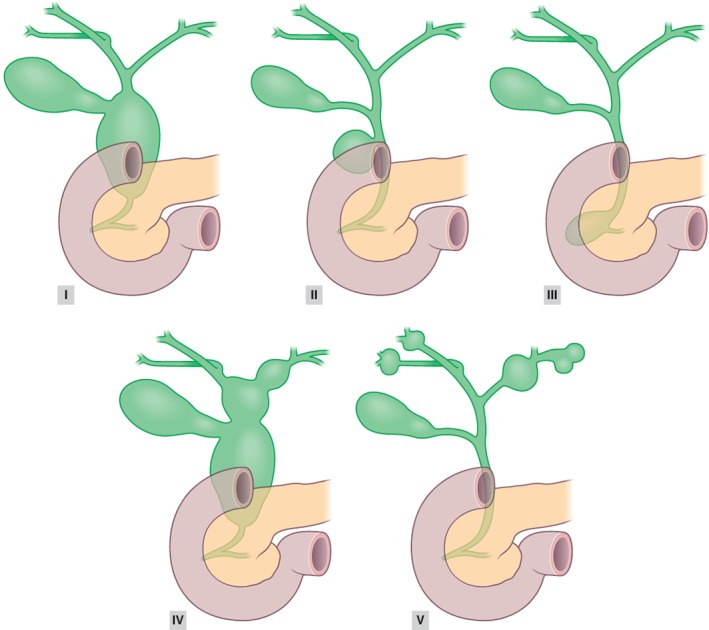
Background: Choledochal malformations comprise various congenital cystic dilatations of the extrahepatic and/or intrahepatic biliary tree. Choledochal malformation is generally considered a premalignant condition, but reliable data on the risk of malignancy and optimal surgical treatment are lacking. The objective of this systematic review was to assess the prevalence of malignancy in patients with choledochal malformation and to differentiate between subtypes. In addition, the risk of malignancy following cystic drainage versus complete cyst excision was assessed.
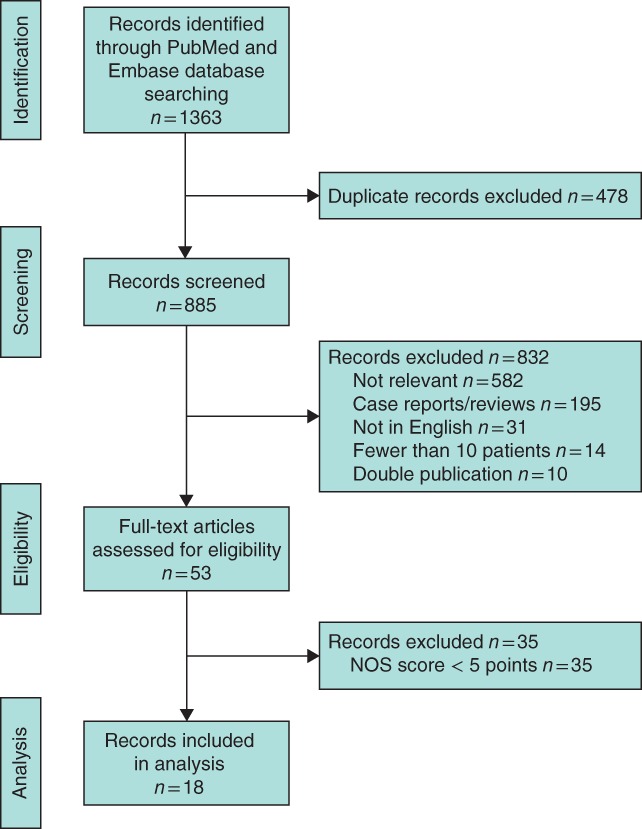
Methods: A systematic review of PubMed and Embase databases was performed in accordance with the PRISMA statement. A meta-analysis of the risk of malignancy following cystic drainage versus complete cyst excision was undertaken in line with MOOSE guidelines. Prevalence of malignancy was defined as the rate of biliary cancer before resection, and malignant transformation as new-onset biliary cancer after surgery.
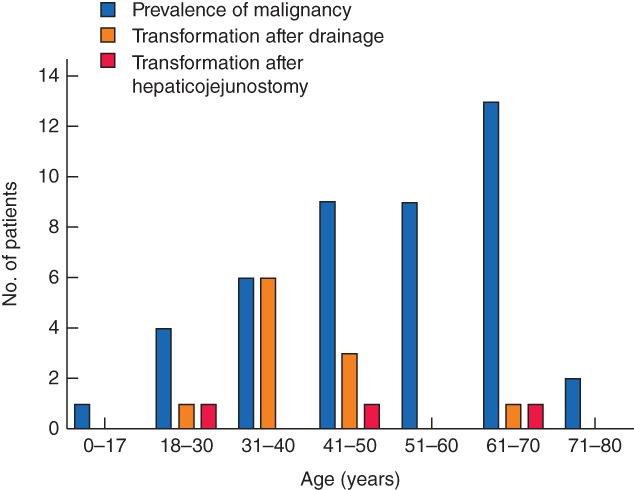
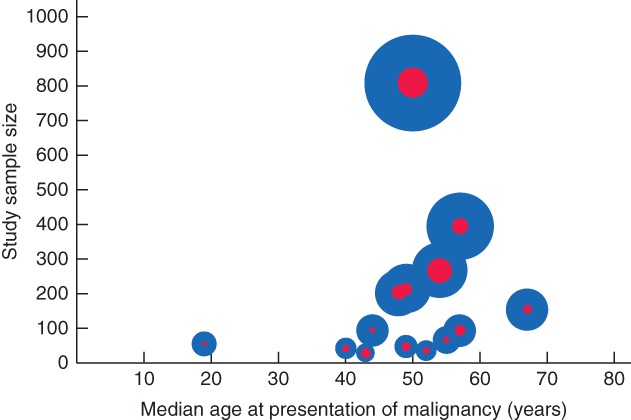
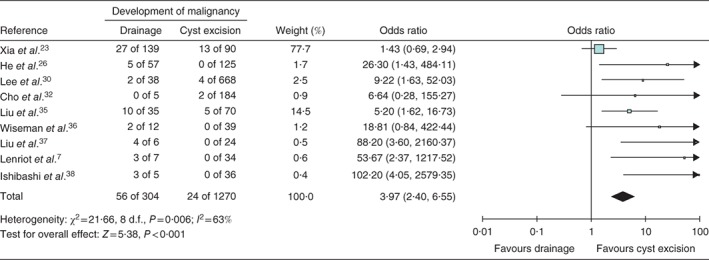
Results: Eighteen observational studies were included, reporting a total of 2904 patients with a median age of 36 years. Of these, 312 in total developed a malignancy (10·7 per cent); the prevalence of malignancy was 7·3 per cent and the rate of malignant transformation was 3·4 per cent. Patients with types I and IV choledochal malformation had an increased risk of malignancy (P = 0·016). Patients who underwent cystic drainage had an increased risk of developing biliary malignancy compared with those who had complete cyst excision, with an odds ratio of 3·97 (95 per cent c.i. 2·40 to 6·55).
Conclusion: The risk of developing malignancy among patients with choledochal malformation was almost 11 per cent. The malignancy risk following cystic drainage surgery was four times higher than that after complete cyst excision. Complete surgical resection is recommended in patients with choledochal malformation.
© 2018 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Makin E, Davenport M. Understanding choledochal malformation. Arch Dis Child 2012; 97: 69–72. - PubMed
-
- Turowski C, Knisely A, Davenport M. Role of pressure and pancreatic reflux in the aetiology of choledochal malformation. Br J Surg 2011; 98: 1319–1326. - PubMed
-
- Kamisawa T, Okamoto A, Tsuruta K, Tu Y, Egawa N. Carcinoma arising in congenital choledochal cysts. Hepatogastroenterology 2008; 55: 329–332. - PubMed
-
- Todani T, Watanabe Y, Narusue M, Tabuchi K, Okajima K. Congenital bile duct cysts: classification, operative procedures, and review of thirty‐seven cases including cancer arising from choledochal cyst. Am J Surg 1977; 134: 263–269. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
