

Surgeon Personal Protection: An Underappreciated Benefit of Positive-pressure Exhaust Suits
- PMID: 29481350
- PMCID: PMC6263565
- DOI: 10.1007/s11999.0000000000000253
Surgeon Personal Protection: An Underappreciated Benefit of Positive-pressure Exhaust Suits
Abstract
Background: Positive-pressure exhaust suits cost more than standard surgical gowns, and recent evidence suggests that they do not decrease infection risk. As a result, some hospitals and surgeons have abandoned positive-pressure exhaust suits in favor of less expensive alternatives. We propose that in addition to their original purpose of decreasing infection rates, positive-pressure exhaust suits may also improve personal protection for the surgeon and assistants, perhaps justifying their added costs.
Questions/purposes: (1) Do positive-pressure exhaust suits decrease exposure to particulate matter during TKA? (2) What areas covered by gowning systems are at risk of exposure to particulate matter?
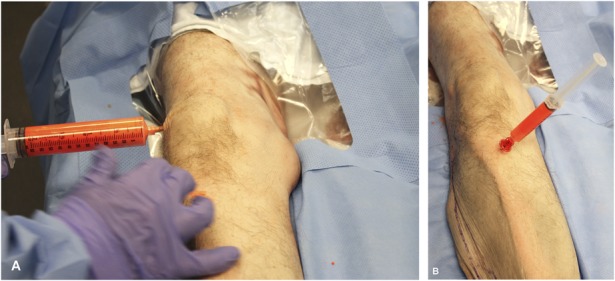
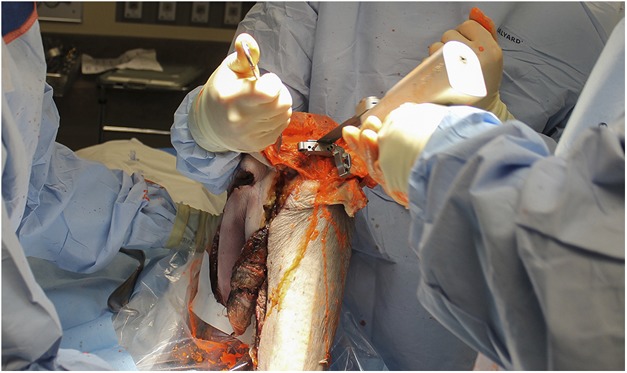
Methods: Three surgical gowning systems were tested: (1) surgical gown, face mask, surgical skull cap, protective eyewear; (2) surgical gown, face mask, surgical protective hood, protective eyewear; and (3) positive-pressure exhaust suit. For each procedure, a cadaver knee was injected intraarticularly and intraosseously with a 5-µm fluorescent powder mixed with water (1 g/10 mL). After gowning in the standard sterile fashion, the primary surgeon and two assistants performed two TKAs with each gowning system for a total of six TKAs. After each procedure, three independent observers graded skin exposure of each surgical participant under ultraviolet light using a standardized scale from 0 (no exposure) to 4 (gross exposure). Statistical analysis was performed using Friedman's and Nemenyi tests. The interrater reliability for the independent observers was also calculated.
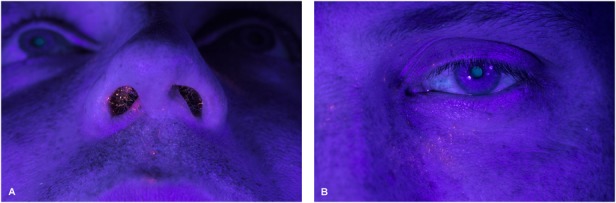
Results: The positive-pressure exhaust suits had less surgeon and assistant exposure compared with other systems (p < 0.001). The median overall exposure grade for each gowning system was 4 for System 1 (range, 3-4), 2.5 for System 2 (range, 2-3), and 0 for System 3 (range, 0-0). In pairwise comparisons between gowning systems, the positive-pressure exhaust suits had less exposure than gowning System 1 (difference of medians: 4, p < 0.001) and gowning System 2 (difference of medians: 2.5, p = 0.038). There was no difference found in exposure between Systems 1 and 2 (difference of medians: 1.5, p = 0.330). When gowning Systems 1 and 2 were removed, particulate matter was found in places that were covered such as the surgeon's beard, lips, inside the nostrils, behind the protective eyewear around the surgeon's eye, and in both eyebrows and eyelashes.
Conclusions: The positive-pressure exhaust suits provided greater personal protection with each procedure than the other two gowning systems.
Clinical relevance: With conventional gowns, particulate matter was found in the surgeon's eyelashes, under the face mask around the mouth, and inside the nostrils. Despite recent evidence that certain types of positive-pressure exhaust suits may not decrease infection, there is a clear benefit of surgeon protection from potentially infectious and harmful patient substances. Despite their added costs, hospitals and surgeons should weigh this protective benefit when considering the use of positive-pressure exhaust suits.
Conflict of interest statement
Each author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures


Comment in
-
CORR Insights®: Surgeon Personal Protection: An Underappreciated Benefit of Positive-pressure Exhaust Suits.Clin Orthop Relat Res. 2018 Jun;476(6):1349-1351. doi: 10.1097/01.blo.0000533609.68604.07. Clin Orthop Relat Res. 2018. PMID: 29698309 Free PMC article. No abstract available.
References
-
- Baffoy-Fayard N, Maugat S, Sapoval M, Cluzel P, Denys A, Sellier N, Desruennes E, Legmann P, Thibault V, Brücker G, Astagneau P; Study Group on Hygiene Practices in Interventional Radiology. Potential exposure to hepatitis C virus through accidental blood contact in interventional radiology. J Vasc Interv Radiol. 2003;14:173–179. - PubMed
-
- Bohn WW, McKinsey DS, Dykstra M, Koppe S. The effect of a portable HEPA-filtered body exhaust system on airborne microbial contamination in a conventional operating room. Infect Control Hosp Epidemiol. 1996;17:419–422. - PubMed
-
- Collins D, Rice J, Nicholson P, Barry K. Quantification of facial contamination with blood during orthopaedic procedures. J Hosp Infect. 2000;45:73–75. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
