

doi: 10.1093/eurheartj/ehy080.
European Society of Cardiology, acute cardiovascular care association, SCAD study group: a position paper on spontaneous coronary artery dissection
Collaborators,
Affiliations
- PMID: 29481627
- PMCID: PMC6148526
- DOI: 10.1093/eurheartj/ehy080
Item in Clipboard
European Society of Cardiology, acute cardiovascular care association, SCAD study group: a position paper on spontaneous coronary artery dissection
Eur Heart J.
.
No abstract available
Figures

Schematic illustration of spontaneous coronary artery dissection. Accumulation and axial propagation of blood forms a false lumen in the outer third of the tunica media leading to external compression of the true lumen (A). Blood may enter through an endothelial-intimal disruption or ‘tear’ (B) or as a result of bleeding from a microvessel within the vessel wall (C) leading to an expanding and compressing false lumen (dotted arrows).
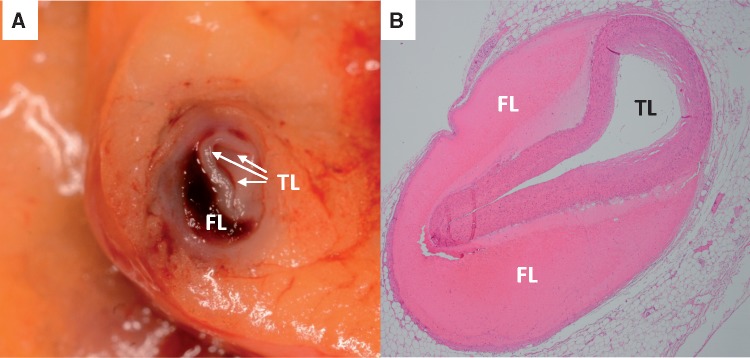
Gross pathology (A) and histopathology (B) showing spontaneous coronary artery dissection with external compression of the true lumen by blood within a false lumen in the outer third of the tunica media.

Extracoronary abnormalities in spontaneous coronary artery dissection including renal (A and D) and femoral (B) fibromuscular dysplasia, carotid and vertebrobasilar aneurysms and tortuosity (C and F) and a localised iliac dissection (E).

Prevalence of extracoronary lesions of fibromuscular dysplasia in contemporary series of spontaneous coronary artery dissection patients.
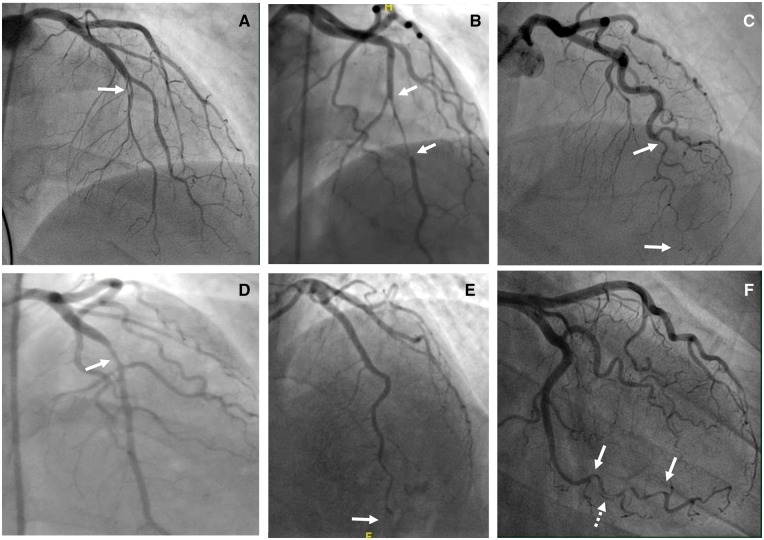
Angiographic classification of spontaneous coronary artery dissection. Type 1 spontaneous coronary artery dissection (A), Type 2A spontaneous coronary artery dissection (B), Type 2B spontaneous coronary artery dissection (C), Type 3 spontaneous coronary artery dissection (D), Type 4 spontaneous coronary artery dissection (E), and Intermediate Type1/2 spontaneous coronary artery dissection (F).

Multivessel spontaneous coronary artery dissection affecting two branches of the circumflex coronary artery, the left anterior descending coronary artery and its diagonal branch (arrows).
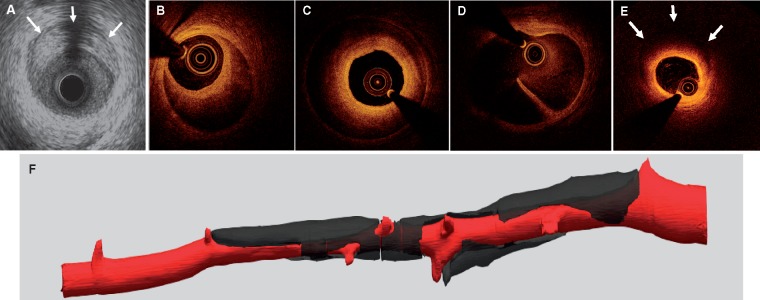
Intracoronary imaging of spontaneous coronary artery dissection by intravascular ultrasound (with outer border of false lumen arrowed, A), and optical coherence tomography showing partial (B) and circumferential (C) false lumens; the site of a fenestration (D) connecting true and false lumens and reduced light penetration through the false lumen (E). Three-dimensional image derived from segmentation of optical coherence tomography image showing how the false lumen tracks around the true lumen and is influenced (and frequently bounded) by side branches (F).

Guidewire passage into the false lumen demonstrated by optical coherence tomography, with both wire (GW) and optical coherence tomography catheter (C) seen in the false lumen outside the compressed true lumen.

Coronary computed tomography findings with parallel angiographic images for a Type 2A dissection of the left anterior descending coronary artery at presentation (A) and following healing after 3-months follow-up (B).

False lumen propagation during stenting. A Type 2A dissection affecting a high obtuse marginal branch of the circumflex but with maintained distal flow (A). Stenting (B) leads to proximal haematoma migration (arrowed C). Two further stents were required in this case to fully exclude the haematoma from luminal restriction.
References
-
- Saw J, Mancini GB, Humphries KH.. Contemporary review on spontaneous coronary artery dissection. J Am Coll Cardiol 2016;68:297–312. - PubMed
-
- Tweet MS, Gulati R, Hayes SN.. Spontaneous coronary artery dissection. Curr Cardiol Rep 2016;18:60.. - PubMed
-
- Tweet MS, Eleid MF, Best PJ, Lennon RJ, Lerman A, Rihal CS, Holmes DR Jr., Hayes SN, Gulati R.. Spontaneous coronary artery dissection: revascularization versus conservative therapy. Circ Cardiovasc Interv 2014;7:777–786. - PubMed
-
- Saw J, Aymong E, Sedlak T, Buller CE, Starovoytov A, Ricci D, Robinson S, Vuurmans T, Gao M, Humphries K, Mancini GB.. Spontaneous coronary artery dissection: association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes. Circ Cardiovasc Interv 2014;7:645–655. - PubMed
-
- Lettieri C, Zavalloni D, Rossini R, Morici N, Ettori F, Leonzi O, Latib A, Ferlini M, Trabattoni D, Colombo P, Galli M, Tarantini G, Napodano M, Piccaluga E, Passamonti E, Sganzerla P, Ielasi A, Coccato M, Martinoni A, Musumeci G, Zanini R, Castiglioni B.. Management and long-term prognosis of spontaneous coronary artery dissection. Am J Cardiol 2015;116:66–73. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
