

Determinants of Diuretic Responsiveness and Associated Outcomes During Acute Heart Failure Hospitalization: An Analysis From the NHLBI Heart Failure Network Clinical Trials
- PMID: 29482026
- PMCID: PMC6102061
- DOI: 10.1016/j.cardfail.2018.02.002
Determinants of Diuretic Responsiveness and Associated Outcomes During Acute Heart Failure Hospitalization: An Analysis From the NHLBI Heart Failure Network Clinical Trials
Abstract
Background: Poor response to loop diuretic therapy is a marker of risk during heart failure hospitalization. We sought to describe baseline determinants of diuretic response and to further explore the relationship between this response and clinical outcomes.
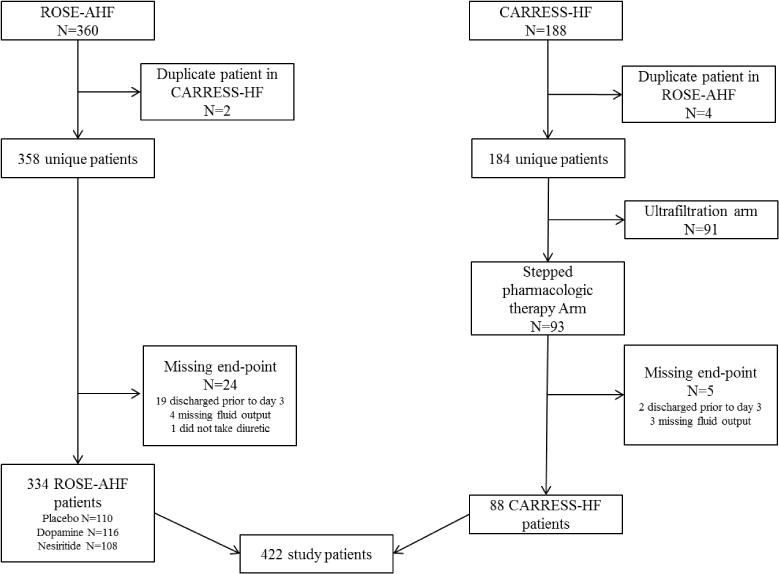
Methods and results: Patient data from the National Heart, Lung, and Blood Institute Heart Failure Network ROSE-AHF and CARRESS-HF clinical trials were analyzed to determine baseline determinants of diuretic response. Diuretic efficiency (DE) was defined as total 72-hour fluid output per total equivalent loop diuretic dose. Data from DOSE-AHF was then used to determine if these predictors of DE correlated with response to a high- versus low-dose diuretic strategy. At 72 hours, the high-DE group had median fluid output of 9071 ml (interquartile range: 7240-11775) with median furosemide dose of 320 mg (220-480) compared with 8030 ml (6300-9915) and 840 mg (600-1215) respectively for the low DE group. Cystatin C was independently associated with DE (odds ratio 0.36 per 1mg/L increase; 95% confidence interval: 0.24-0.56; P < 0.001). Independently from baseline characteristics, reduced fluid output, weight loss and DE were each associated with increased 60 day mortality. Among patients with estimated glomerular filtration rate below the median, those randomized to a high-dose strategy had improved symptoms compared with those randomized to a low-dose strategy.
Conclusions: Elevated baseline cystatin C, as a biomarker of renal dysfunction, is associated with reduced diuretic response during heart failure hospitalization. Higher loop diuretic doses are required for therapeutic decongestion in patients with renal insufficiency. Poor response identifies a high-risk population.
Keywords: Acute heart failure; congestion; cystatin C; loop diuretic; renal failure.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures



Comment in
-
Efficient, Efficacious, Effective: Still a Long Way to Go for Diuretic Treatment of Acute Decompensated Heart Failure.J Card Fail. 2018 Jul;24(7):439-441. doi: 10.1016/j.cardfail.2018.06.002. Epub 2018 Jun 25. J Card Fail. 2018. PMID: 29953939 No abstract available.
References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013 Oct 15;128(16):1810–52. - PubMed
-
- Bettencourt P, Azevedo A, Pimenta J, Frioes F, Ferreira S, Ferreira A. N-terminal-pro-brain natriuretic peptide predicts outcome after hospital discharge in heart failure patients. Circulation. 2004 Oct 12;110(15):2168–74. - PubMed
-
- Lucas C, Johnson W, Hamilton MA, Fonarow GC, Woo MA, Flavell CM, et al. Freedom from congestion predicts good survival despite previous class IV symptoms of heart failure. Am Heart J. 2000 Dec;140(6):840–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
