

Unrecognized Cardiovascular Emergencies Among Medicare Patients
- PMID: 29482196
- PMCID: PMC5876812
- DOI: 10.1001/jamainternmed.2017.8628
Unrecognized Cardiovascular Emergencies Among Medicare Patients
Abstract
Importance: The Institute of Medicine described diagnostic error as the next frontier in patient safety and highlighted a critical need for better measurement tools.
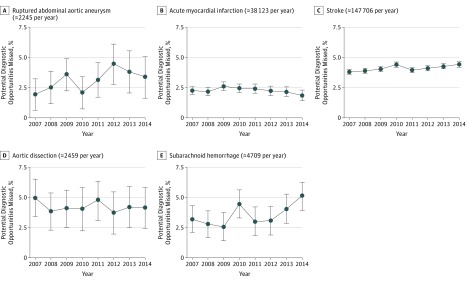
Objectives: To estimate the proportions of emergency department (ED) visits attributable to symptoms of imminent ruptured abdominal aortic aneurysm (AAA), acute myocardial infarction (AMI), stroke, aortic dissection, and subarachnoid hemorrhage (SAH) that end in discharge without diagnosis; to evaluate longitudinal trends; and to identify patient characteristics independently associated with missed diagnostic opportunities.
Design, setting, and participants: This was a retrospective cohort study of all Medicare claims for 2006 to 2014. The setting was hospital EDs in the United States. Participants included all fee-for-service Medicare patients admitted to the hospital during 2007 to 2014 for the conditions of interest. Hospice enrollees and patients with recent skilled nursing facility stays were excluded.
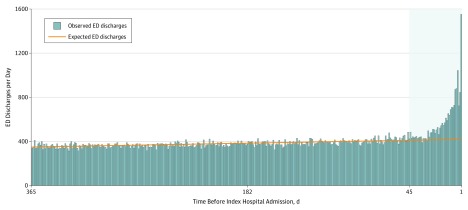
Main outcomes and measures: The proportion of potential diagnostic opportunities missed in the ED was estimated using the difference between observed and expected ED discharges within 45 days of the index hospital admissions as the numerator, basing expected discharges on ED use by the same patients in earlier months. The denominator was estimated as the number of recognized emergencies (index hospital admissions) plus unrecognized emergencies (excess discharges).
Results: There were 1 561 940 patients, including 17 963 hospitalized for ruptured AAA, 304 980 for AMI, 1 181 648 for stroke, 19 675 for aortic dissection, and 37 674 for SAH. The mean (SD) age was 77.9 (10.3) years; 8.9% were younger than 65 years, and 54.1% were female. The proportions of diagnostic opportunities missed in the ED were as follows: ruptured AAA (3.4%; 95% CI, 2.9%-4.0%), AMI (2.3%; 95% CI, 2.1%-2.4%), stroke (4.1%; 95% CI, 4.0%-4.2%), aortic dissection (4.5%; 95% CI, 3.9%-5.1%), and SAH (3.5%; 95% CI, 3.1%-3.9%). Longitudinal trends were either nonsignificant (AMI and aortic dissection) or increasing (ruptured AAA, stroke, and SAH). Patient characteristics associated with unrecognized emergencies included age younger than 65 years, dual eligibility for Medicare and Medicaid coverage, female sex, and each of the following chronic conditions: end-stage renal disease, dementia, depression, diabetes, cerebrovascular disease, hypertension, coronary artery disease, and chronic obstructive pulmonary disease.
Conclusions and relevance: Among Medicare patients, opportunities to diagnose ruptured AAA, AMI, stroke, aortic dissection, and SAH are missed in less than 1 in 20 ED presentations. Further improvement may prove difficult.
Conflict of interest statement
Figures
References
-
- Institute of Medicine, National Academies of Sciences, Engineering, and Medicine Improving Diagnosis in Health Care. Washington, DC: National Academies Press; 2015.
-
- McGlynn EA, McDonald KM, Cassel CK. Measurement is essential for improving diagnosis and reducing diagnostic error: a report from the Institute of Medicine. JAMA. 2015;314(23):2501-2502. - PubMed
-
- Research Data Assistance Center How to identify hospital claims for emergency room visits in the Medicare claims data. https://www.resdac.org/resconnect/articles/144. Published July 30, 2015. Accessed January 23, 2018.
-
- Centers for Medicare & Medicaid Services Chronic Conditions Data Warehouse. https://www.ccwdata.org/web/guest/condition-categories. Accessed July 20, 2017.
-
- Pope JH, Aufderheide TP, Ruthazer R, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000;342(16):1163-1170. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
