

Baseline autoantibody profile in rheumatoid arthritis is associated with early treatment response but not long-term outcomes
- PMID: 29482627
- PMCID: PMC5828136
- DOI: 10.1186/s13075-018-1520-4
Baseline autoantibody profile in rheumatoid arthritis is associated with early treatment response but not long-term outcomes
Abstract
Background: The autoantibody profile of seropositive rheumatoid arthritis (RA) is very diverse and consists of various isotypes and antibodies to multiple post-translational modifications. It is yet unknown whether this varying breadth of the autoantibody profile is associated with treatment outcomes. Therefore, we investigated whether the composition of the autoantibody profile in RA, as a marker of the underlying immunopathology, influences initial and long-term treatment outcomes.
Methods: In serum from 399 seropositive patients with RA in the IMPROVED study, drawn at baseline and at the moment of drug tapering, we measured IgG, IgM, and IgA isotypes for anti-cyclic citrullinated peptide-2 and anti-carbamylated protein antibodies, IgM and IgA rheumatoid factor, and reactivity against four citrullinated and two acetylated peptides (anti-modified protein antibodies (AMPAs)). We investigated the effect of the breadth of the autoantibody profile on (1) change in disease activity score (DAS)44 between 0 and 4 months, (2) initial drug-free remission (DFR, drug-free DAS44 < 1.6) achieved between 1 and 2 years of follow up, and (3) long-term sustained DFR until last follow up.
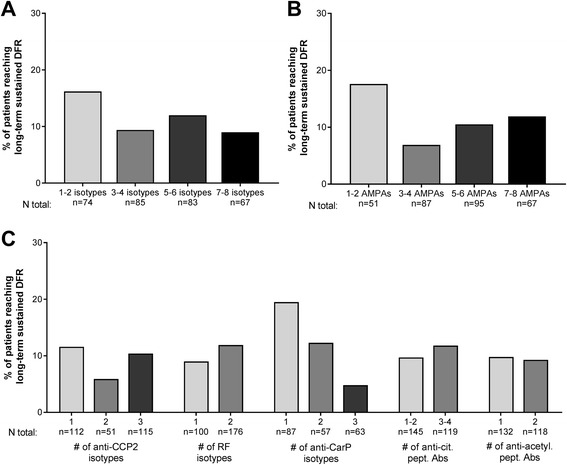
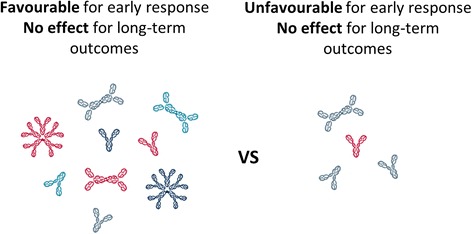
Results: Patients with a broad autoantibody profile at baseline had a significantly better early treatment response: ΔDAS 0-4 months of 1-2, 3-4, and 5-6 vs 7-8 isotypes, -1.5 (p < 0.001), -1.7 (p = 0.03), and -1.8 (p = 0.04) vs -2.2. Similar results were observed for AMPA number. However, patients with a broad baseline autoantibody profile achieved less initial DFR. For long-term sustained DFR there was no longer an association with the breadth of the autoantibody response. When assessing autoantibodies at the moment of tapering, similar trends were observed.
Conclusions: A broad baseline autoantibody profile is associated with a better early treatment response. The breadth of the baseline autoantibody profile, reflecting a break in tolerance against several different autoantigens and extensive isotype switching, may indicate a more active humoral autoimmunity, which could make the underlying disease processes initially more suppressible by medication. The lack of association with long-term sustained DFR suggests that the relevance of the baseline autoantibody profile diminishes over time.
Trial registration: ISRCTN11916566 . Registered on 7 November 2006. EudraCT, 2006- 06186-16. Registered on 16 July 2007.
Keywords: Ant-CCP; Autoantibodies; Disease activity; Rheumatoid arthritis; Rheumatoid factor.
Conflict of interest statement
Ethics approval and consent to participate
This study was conducted with the approval of the regional ethics committee at Leiden University Medical Center. The IMPROVED study was approved by the Medical Ethics Committees of all participating hospitals. Informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures




References
-
- Haschka J, Englbrecht M, Hueber AJ, Manger B, Kleyer A, Reiser M, et al. Relapse rates in patients with rheumatoid arthritis in stable remission tapering or stopping antirheumatic therapy: interim results from the prospective randomised controlled RETRO study. Ann Rheum Dis. 2016;75:45–51. doi: 10.1136/annrheumdis-2014-206439. - DOI - PubMed
-
- Heimans L, Akdemir G, Boer KV, Goekoop-Ruiterman YP, Molenaar ET, van Groenendael JH, et al. Two-year results of disease activity score (DAS)-remission-steered treatment strategies aiming at drug-free remission in early arthritis patients (the IMPROVED-study) Arthritis Res Ther. 2016;18:23. doi: 10.1186/s13075-015-0912-y. - DOI - PMC - PubMed
-
- van der Kooij SM, Goekoop-Ruiterman YP, de Vries-Bouwstra JK, Guler-Yuksel M, Zwinderman AH, Kerstens PJ, et al. Drug-free remission, functioning and radiographic damage after 4 years of response-driven treatment in patients with recent-onset rheumatoid arthritis. Ann Rheum Dis. 2009;68:914–21. doi: 10.1136/ard.2008.092254. - DOI - PubMed
-
- van der Woude D, Young A, Jayakumar K, Mertens BJ, Toes RE, van der Heijde D, et al. Prevalence of and predictive factors for sustained disease-modifying antirheumatic drug-free remission in rheumatoid arthritis: results from two large early arthritis cohorts. Arthritis Rheum. 2009;60:2262–71. doi: 10.1002/art.24661. - DOI - PubMed
-
- Wevers-de Boer K, Visser K, Heimans L, Ronday HK, Molenaar E, Groenendael JH, et al. Remission induction therapy with methotrexate and prednisone in patients with early rheumatoid and undifferentiated arthritis (the IMPROVED study) Ann Rheum Dis. 2012;71:1472–7. doi: 10.1136/annrheumdis-2011-200736. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
