

The effects of acceptance and commitment therapy on eating behavior and diet delivered through face-to-face contact and a mobile app: a randomized controlled trial
- PMID: 29482636
- PMCID: PMC5828146
- DOI: 10.1186/s12966-018-0654-8
The effects of acceptance and commitment therapy on eating behavior and diet delivered through face-to-face contact and a mobile app: a randomized controlled trial
Abstract
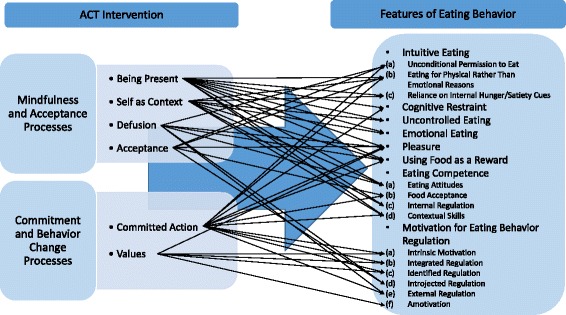
Background: Internal motivation and good psychological capabilities are important factors in successful eating-related behavior change. Thus, we investigated whether general acceptance and commitment therapy (ACT) affects reported eating behavior and diet quality and whether baseline perceived stress moderates the intervention effects.
Methods: Secondary analysis of unblinded randomized controlled trial in three Finnish cities. Working-aged adults with psychological distress and overweight or obesity in three parallel groups: (1) ACT-based Face-to-face (n = 70; six group sessions led by a psychologist), (2) ACT-based Mobile (n = 78; one group session and mobile app), and (3) Control (n = 71; only the measurements). At baseline, the participants' (n = 219, 85% females) mean body mass index was 31.3 kg/m2 (SD = 2.9), and mean age was 49.5 years (SD = 7.4). The measurements conducted before the 8-week intervention period (baseline), 10 weeks after the baseline (post-intervention), and 36 weeks after the baseline (follow-up) included clinical measurements, questionnaires of eating behavior (IES-1, TFEQ-R18, HTAS, ecSI 2.0, REBS), diet quality (IDQ), alcohol consumption (AUDIT-C), perceived stress (PSS), and 48-h dietary recall. Hierarchical linear modeling (Wald test) was used to analyze the differences in changes between groups.
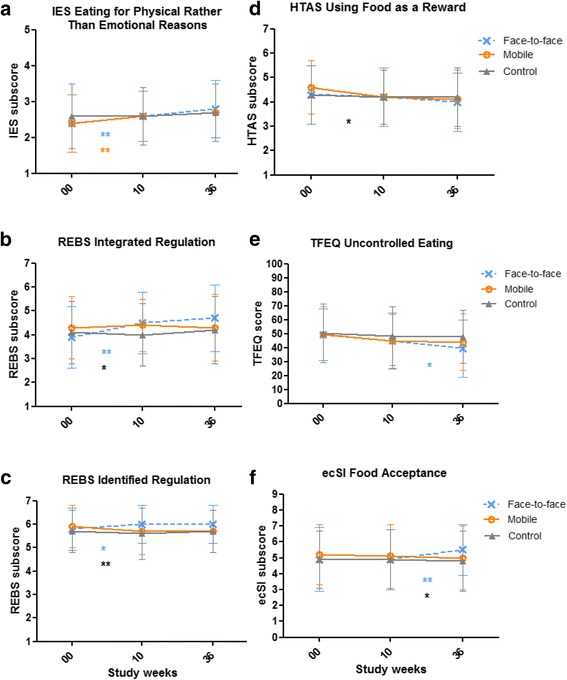
Results: Group x time interactions showed that the subcomponent of intuitive eating (IES-1), i.e., Eating for physical rather than emotional reasons, increased in both ACT-based groups (p = .019); the subcomponent of TFEQ-R18, i.e., Uncontrolled eating, decreased in the Face-to-face group (p = .020); the subcomponent of health and taste attitudes (HTAS), i.e., Using food as a reward, decreased in the Mobile group (p = .048); and both subcomponent of eating competence (ecSI 2.0), i.e., Food acceptance (p = .048), and two subcomponents of regulation of eating behavior (REBS), i.e., Integrated and Identified regulation (p = .003, p = .023, respectively), increased in the Face-to-face group. Baseline perceived stress did not moderate effects on these particular features of eating behavior from baseline to follow-up. No statistically significant effects were found for dietary measures.
Conclusions: ACT-based interventions, delivered in group sessions or by mobile app, showed beneficial effects on reported eating behavior. Beneficial effects on eating behavior were, however, not accompanied by parallel changes in diet, which suggests that ACT-based interventions should include nutritional counseling if changes in diet are targeted.
Trial registration: ClinicalTrials.gov ( NCT01738256 ), registered 17 August, 2012.
Keywords: ACT; Behavior change; Dietary intake; Intuitive eating; Mindful eating; Mindfulness; Obesity; Overweight; Regulation of eating behavior; mHealth.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the ethics committee of the Central Finland Health Care District (reference number 7 U/2012) and was performed in accordance with the Declaration of Helsinki. The participants gave their written informed consent before participating.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Samdal GB, Eide GE, Barth T, Williams G, Meland E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int J Behav Nutr Phys Act. 2017;14:42. doi: 10.1186/s12966-017-0494-y. - DOI - PMC - PubMed
-
- Pelletier LG, Dion SC, Slovinec-D’Angelo M, Reid R. Why do you regulate what you eat? Relationships between forms of regulation, eating behaviors, sustained dietary behavior change, and psychological adjustment. Motiv Emot. 2004;28:245–277. doi: 10.1023/B:MOEM.0000040154.40922.14. - DOI
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
