

Review
doi: 10.1016/j.ijrobp.2017.12.290.
Epub 2018 Jan 6.
Radiation Dose-Volume Effects for Liver SBRT
Affiliations
- PMID: 29482870
- PMCID: PMC6095822
- DOI: 10.1016/j.ijrobp.2017.12.290
Item in Clipboard
Review
Radiation Dose-Volume Effects for Liver SBRT
Int J Radiat Oncol Biol Phys.
.
Abstract
Stereotactic body radiation therapy (SBRT) has emerged as an effective, noninvasive treatment option for primary liver cancer and metastatic disease occurring in the liver. Although SBRT can be highly effective for establishing local control in hepatic malignancies, a tradeoff exists between tumor control and normal tissue complications. The objective of the present study was to review the normal tissue dose-volume effects for SBRT-induced liver and gastrointestinal toxicities and derive normal tissue complication probability models.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: none.
Figures
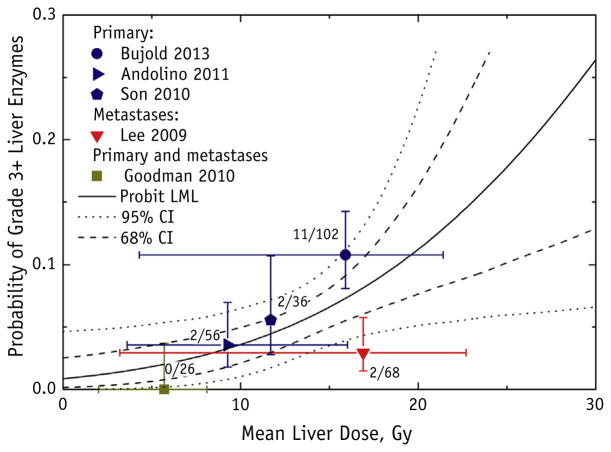
Grade ≥3 liver enzyme toxicity as a function of mean liver dose (MLD), with probit model fit and 95% and 68% confidence intervals (CIs). Dose “error bars” (horizontal axis) for each data point represent range of reported doses for each study; toxicity “error bars” (vertical axis) represent binomial 68% CIs. The number of patients who developed toxicity of the total number of patients for each study is displayed next to the data point. All studies excluded the gross tumor volume in the MLD calculation, with the exception of Son et al (20). Probit model fitting failed to establish the upper confidence limit for the dose to 50% of the target, and the null hypothesis of no dose response was not rejected (P = .10); therefore, we could not exclude that the incidence of liver enzyme complications was independent of the dose; the probit model fit is displayed for reference. Abbreviation: LML = log maximum likelihood.
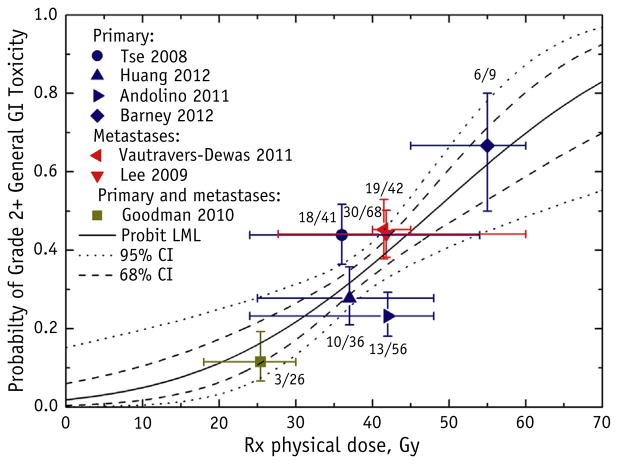
Grade ≥2 general gastrointestinal (GI) toxicity as a function of the prescription (Rx) physical dose to the target, with the probit model result (maximum likelihood parameter fitting) and 95% and 68% confidence intervals (CIs). General GI toxicities were defined as fatigue, nausea, diarrhea, gastritis, ulcers, GI area pain, and colitis. The target Rx dose definition is provided in Table 2. Each data point was placed at the reported mean or median dose and reported complication rate; horizontal error bars represent the reported ranges, and the vertical error bars represent binomial 68% CIs. The number of patients who developed toxicity of the total number of patients for each study is displayed next to the data point. The study by Andolino et al (14) did not distinguish between grade 1 and 2 general GI toxicities. Abbreviation: LML = log maximum likelihood.
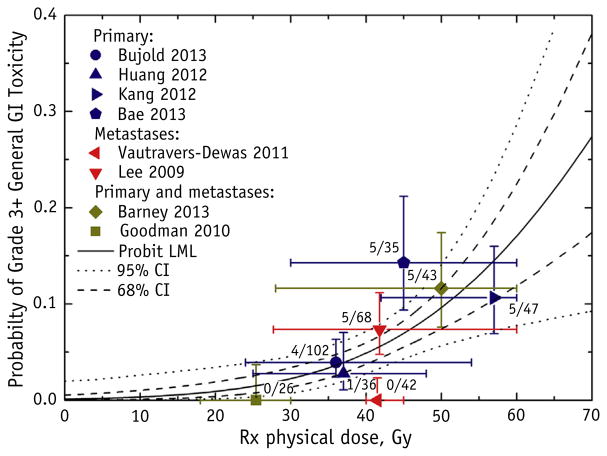
Grade ≥3 general gastrointestinal (GI) toxicity as a function of the prescription (Rx) physical dose to the target, with the probit model result (maximum likelihood parameter fitting) and 95% and 68% confidence intervals (CIs). General GI toxicities were defined as fatigue, nausea, diarrhea, gastritis, ulcers, GI area pain, and colitis. The target RX dose definition is provided in Table 2. Each data point is placed at the reported mean or median dose and reported complication rate; the horizontal error bars represent the reported ranges, and the vertical error bars represent binomial 68% CIs. The number of patients who developed toxicity out of the total number of patients for each study is displayed next to the data point. Abbreviation: LML = log maximum likelihood.
References
-
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: Globocan 2008. Int J Cancer. 2010;127:2893–2917. - PubMed
-
- Paley MR, Ros PR. Hepatic metastases. Radiol Clin North Am. 1998;36:349–363. - PubMed
-
- Fong Y, Cohen AM, Fortner JG, et al. Liver resection for colorectal metastases. J Clin Oncol. 1997;15:938–946. - PubMed
-
- Aloia TA, Vauthey J-N, Loyer EM, et al. Solitary colorectal liver metastasis: Resection determines outcome. Arch Surg. 2006;141:460–467. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
