

A randomized and open-label phase II trial reports the efficacy of neoadjuvant lobaplatin in breast cancer
- PMID: 29483583
- PMCID: PMC5827032
- DOI: 10.1038/s41467-018-03210-2
A randomized and open-label phase II trial reports the efficacy of neoadjuvant lobaplatin in breast cancer
Abstract
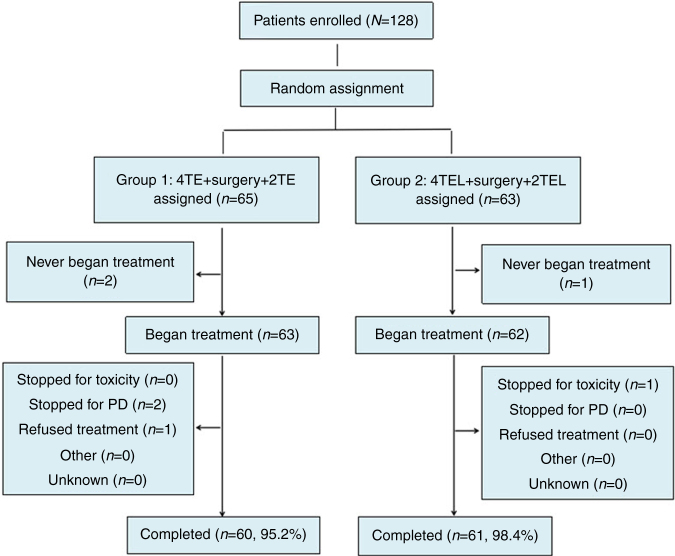
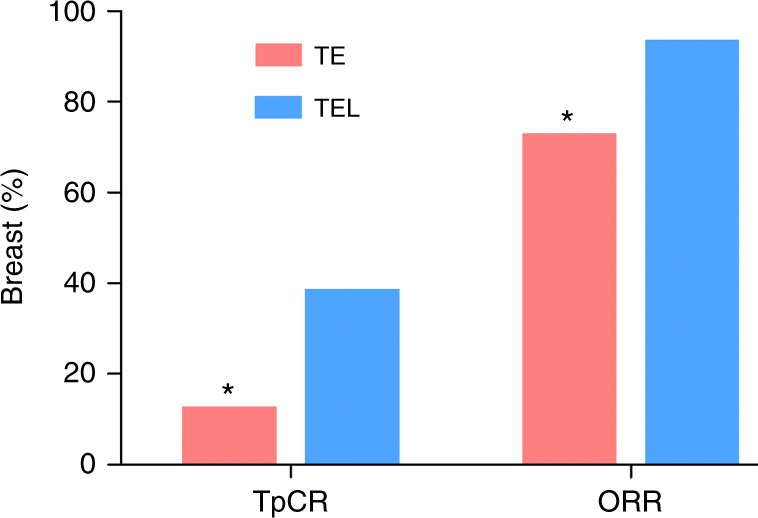
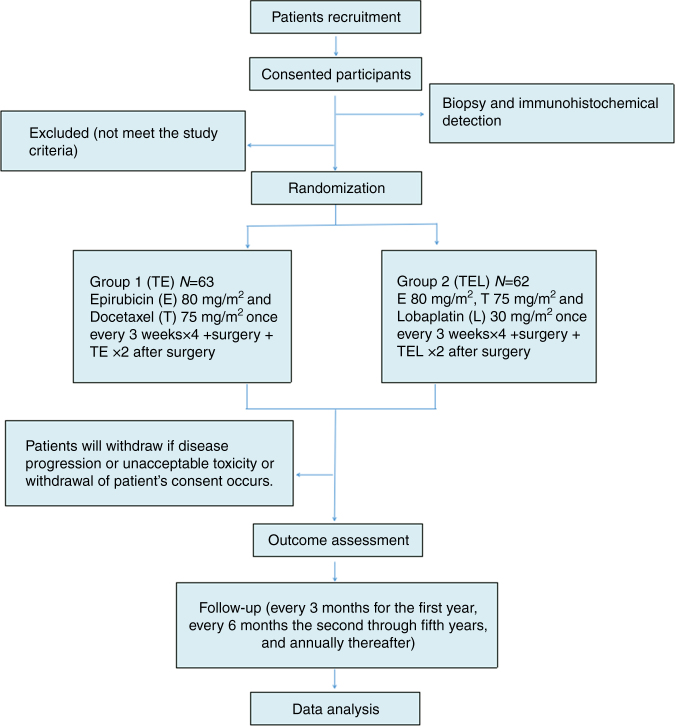
Currently, one sixth of triple-negative breast cancer (TNBC) patients who receive docetaxel (T) and epirubicin (E) as neoadjuvant chemotherapy achieve a pathologic complete response (pCR). This study evaluates the impact of adding lobaplatin (L) to the TE regimen. Here, we show data from 125 patients (63 TE and 62 TEL patients). Four patients did not complete all the cycles. Two-sided P values show that the addition of L (38.7% vs. 12.7%, P = 0.001) significantly increases the rate of pCR in the breast and the axilla (TpCR) and the overall response rate (ORR; 93.5% vs. 73.0%, P = 0.003). The occurrence of grade 3-4 anemia and thrombocytopenia is higher in the TEL group (52.5% vs. 10.0% and 34.4% vs. 1.7% respectively). These results demonstrate that the addition of L to the TE regimen as neoadjuvant chemotherapy improves the TpCR and the ORR rates of TNBC but with increased side effects.
Conflict of interest statement
The authors declare no competing financial interests.
Figures

References
-
- Stover DG, Winer EP. Tailoring adjuvant chemotherapy regimens for patients with triple negative breast cancer. Breast. 2016;Suppl 2:S132–S135. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
