

Acute Kidney Injury in Trauma Patients Admitted to Critical Care: Development and Validation of a Diagnostic Prediction Model
- PMID: 29483607
- PMCID: PMC5827665
- DOI: 10.1038/s41598-018-21929-2
Acute Kidney Injury in Trauma Patients Admitted to Critical Care: Development and Validation of a Diagnostic Prediction Model
Abstract
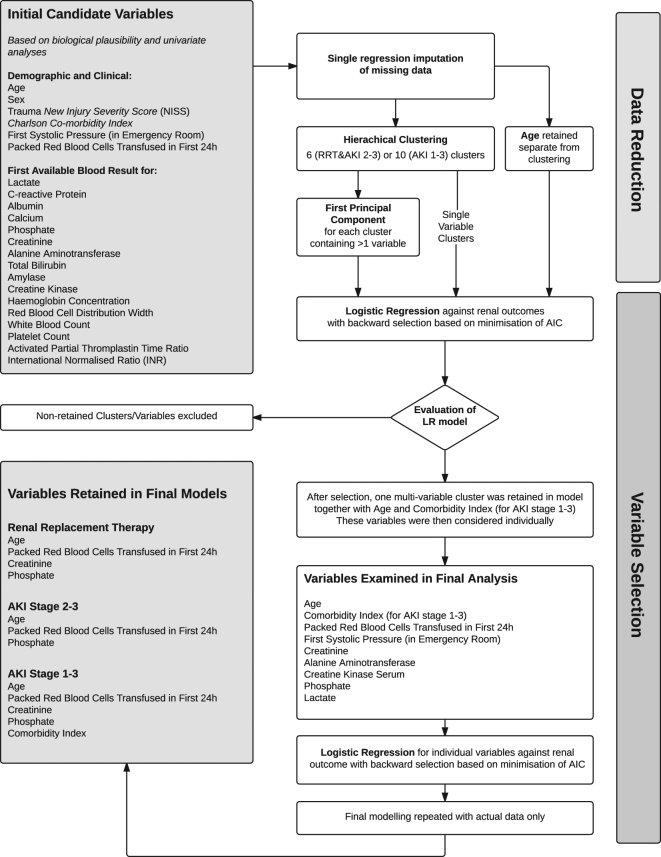
Acute Kidney Injury (AKI) complicating major trauma is associated with increased mortality and morbidity. Traumatic AKI has specific risk factors and predictable time-course facilitating diagnostic modelling. In a single centre, retrospective observational study we developed risk prediction models for AKI after trauma based on data around intensive care admission. Models predicting AKI were developed using data from 830 patients, using data reduction followed by logistic regression, and were independently validated in a further 564 patients. AKI occurred in 163/830 (19.6%) with 42 (5.1%) receiving renal replacement therapy (RRT). First serum creatinine and phosphate, units of blood transfused in first 24 h, age and Charlson score discriminated need for RRT and AKI early after trauma. For RRT c-statistics were good to excellent: development: 0.92 (0.88-0.96), validation: 0.91 (0.86-0.97). Modelling AKI stage 2-3, c-statistics were also good, development: 0.81 (0.75-0.88) and validation: 0.83 (0.74-0.92). The model predicting AKI stage 1-3 performed moderately, development: c-statistic 0.77 (0.72-0.81), validation: 0.70 (0.64-0.77). Despite good discrimination of need for RRT, positive predictive values (PPV) at the optimal cut-off were only 23.0% (13.7-42.7) in development. However, PPV for the alternative endpoint of RRT and/or death improved to 41.2% (34.8-48.1) highlighting death as a clinically relevant endpoint to RRT.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter. Suppl. 2, 1–138 (2012).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
