

Fascia Suture Technique and Suture-mediated Closure Devices: Systematic Review
- PMID: 29483761
- PMCID: PMC5825226
- DOI: 10.1055/s-0037-1620241
Fascia Suture Technique and Suture-mediated Closure Devices: Systematic Review
Abstract
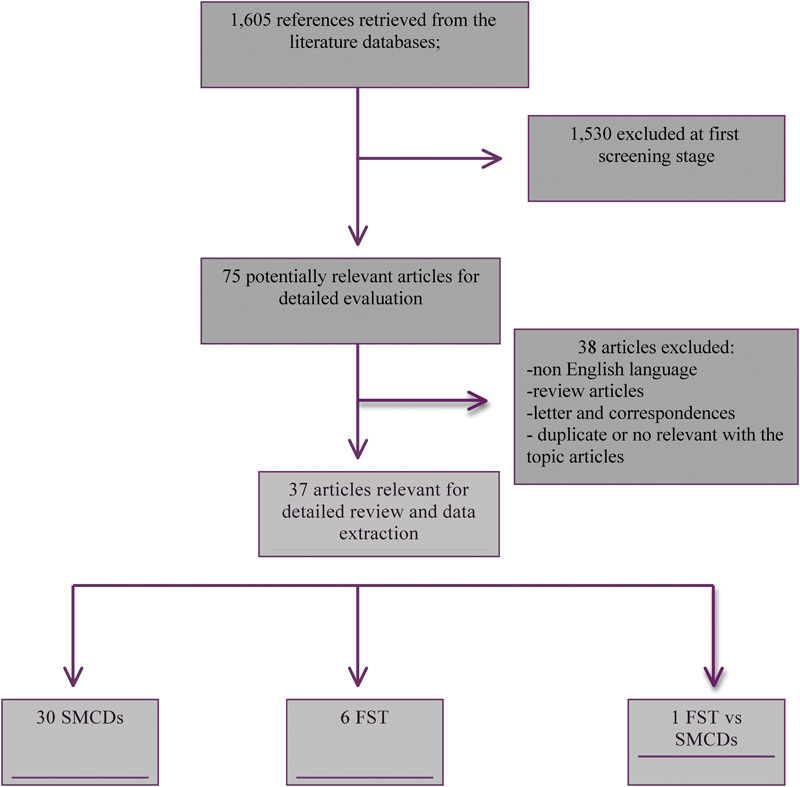
Background The aim of the present study is to review the available data on suture-mediated closure devices (SMCDs) and fascia suture technique (FST), which are alternatives for minimizing the invasiveness of percutaneous endovascular aortic aneurysm repair (p-EVAR) and reduce the complications related to groin dissections. Methods The Medline, ClinicalTrials.gov, and Cochrane library - Cochrane Central Register of Controlled Trials (CENTRAL) databases were searched for publications regarding SMCD and FST between January 1999 and December 2016. Results We review 37 original articles, 30 referring to SMCDs (Prostar XL and Proglide), which included 3,992 patients, and 6 articles referring to FST, which include 426 patients. The two techniques are compared only in one article (100 patients). The two types of SMCDs were Prostar and Proglide. In most studies on SMCDs, the reported technical success rates were between 89 and 100%, but the complication rates varied greatly between 0 and 25%. Concerning FST, the technical success rates were also high, ranging between 87 and 99%. However, intraoperative complication rates ranged between 1.2 and 13%, whereas postoperative complication rates varied from 0.9 to 6.2% for the short-term and from 1.9 to 13.6% for the long-term. Conclusions SMCDs and FST seem to be effective and simple methods for closing common femoral artery (CFA) punctures after p-EVAR. FST can reduce the access closure time and the procedural costs with a quite short learning curve, whereas it can work as a bailout procedure for failed SMCDs suture. The few failures of the SMCDs and FST that may occur due to bleeding or occlusion can easily be managed.
Keywords: Proglide system; Prostar XL; complications; fascia suture technique; femoral access; percutaneous endovascular aortic aneurysm repair; suture-mediated closure devices.
Conflict of interest statement
Figures
References
-
- Birch S E, Borchard K L, Hewitt P M, Stary D, Scott A R. Endovascular abdominal aortic aneurysm repair: a 7 year experience at the Launceston General Hospital. ANZ J Surg. 2005;75(05):302–307. - PubMed
-
- Dalainas I, Nano G, Casana R, Tealdi Dg. Mid-term results after endovascular repair of abdominal aortic aneurysms: a four-year experience. Eur J Vasc Endovasc Surg. 2004;27(03):319–323. - PubMed
-
- Kibbe M R, Matsumura J S; Excluder Investigators.The Gore Excluder US multi-center trial: analysis of adverse events at 2 years Semin Vasc Surg 20031602144–150. - PubMed
-
- Slappy A L, Hakaim A G, Oldenburg W A, Paz-Fumagalli R, McKinney J M. Femoral incision morbidity following endovascular aortic aneurysm repair. Vasc Endovascular Surg. 2003;37(02):105–109. - PubMed
-
- Faries P L, Brener B J, Connelly T L et al.A multicenter experience with the Talent endovascular graft for the treatment of abdominal aortic aneurysms. J Vasc Surg. 2002;35(06):1123–1128. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
