

Randomised controlled trial of simvastatin treatment for autism in young children with neurofibromatosis type 1 (SANTA)
- PMID: 29484149
- PMCID: PMC5824534
- DOI: 10.1186/s13229-018-0190-z
Randomised controlled trial of simvastatin treatment for autism in young children with neurofibromatosis type 1 (SANTA)
Abstract
Background: Neurofibromatosis 1 (NF1) is a monogenic model for syndromic autism. Statins rescue the social and cognitive phenotype in animal knockout models, but translational trials with subjects > 8 years using cognition/behaviour outcomes have shown mixed results. This trial breaks new ground by studying statin effects for the first time in younger children with NF1 and co-morbid autism and by using multiparametric imaging outcomes.
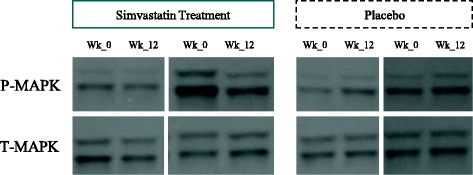
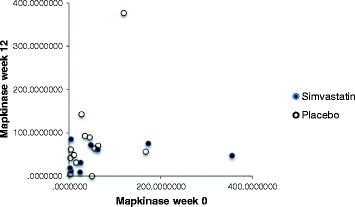
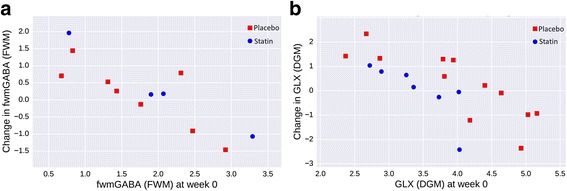
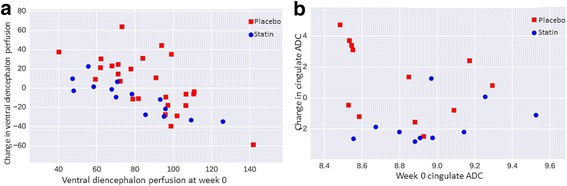
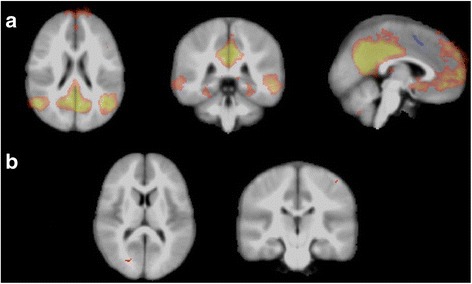
Methods: A single-site triple-blind RCT of simvastatin vs. placebo was done. Assessment (baseline and 12-week endpoint) included peripheral MAPK assay, awake magnetic resonance imaging spectroscopy (MRS; GABA and glutamate+glutamine (Glx)), arterial spin labelling (ASL), apparent diffusion coefficient (ADC), resting state functional MRI, and autism behavioural outcomes (Aberrant Behaviour Checklist and Clinical Global Impression).
Results: Thirty subjects had a mean age of 8.1 years (SD 1.8). Simvastatin was well tolerated. The amount of imaging data varied by test. Simvastatin treatment was associated with (i) increased frontal white matter MRS GABA (t(12) = - 2.12, p = .055), GABA/Glx ratio (t(12) = - 2.78, p = .016), and reduced grey nuclei Glx (ANCOVA p < 0.05, Mann-Whitney p < 0.01); (ii) increased ASL perfusion in ventral diencephalon (Mann-Whitney p < 0.01); and (iii) decreased ADC in cingulate gyrus (Mann-Whitney p < 0.01). Machine-learning classification of imaging outcomes achieved 79% (p < .05) accuracy differentiating groups at endpoint against chance level (64%, p = 0.25) at baseline. Three of 12 (25%) simvastatin cases compared to none in placebo met 'clinical responder' criteria for behavioural outcome.
Conclusions: We show feasibility of peripheral MAPK assay and autism symptom measurement, but the study was not powered to test effectiveness. Multiparametric imaging suggests possible simvastatin effects in brain areas previously associated with NF1 pathophysiology and the social brain network.
Trial registration: EU Clinical Trial Register (EudraCT) 2012-005742-38 (www.clinicaltrialsregister.eu).
Keywords: Autism; Neurofibromatosis type 1; Neuroimaging; Randomised controlled trial; Simvastatin; Statin.
Conflict of interest statement
The study was approved by the National Research Ethics Service Committee North West-Great Manchester Central (reference 13/NW/0111).All data generated or analysed during the study are included in this published article (and its Additional files).D. Gareth Evans had a travel for a trial meeting paid for by the Amgen and declared no other conflicts of interest. All other authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Plasschaert E, Descheemaeker MJ, Van Eylen L, Noens I, Steyaert J, Legius E. Prevalence of autism spectrum disorder symptoms in children with neurofibromatosis type 1. Am J Med Genet B Neuropsychiatr Genet. 2014; - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
