

Hypertension in pregnancy: Taking cues from pathophysiology for clinical practice
- PMID: 29485737
- PMCID: PMC6490052
- DOI: 10.1002/clc.22892
Hypertension in pregnancy: Taking cues from pathophysiology for clinical practice
Abstract
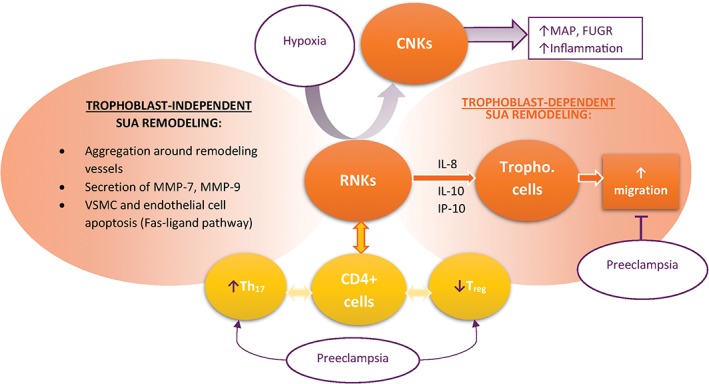
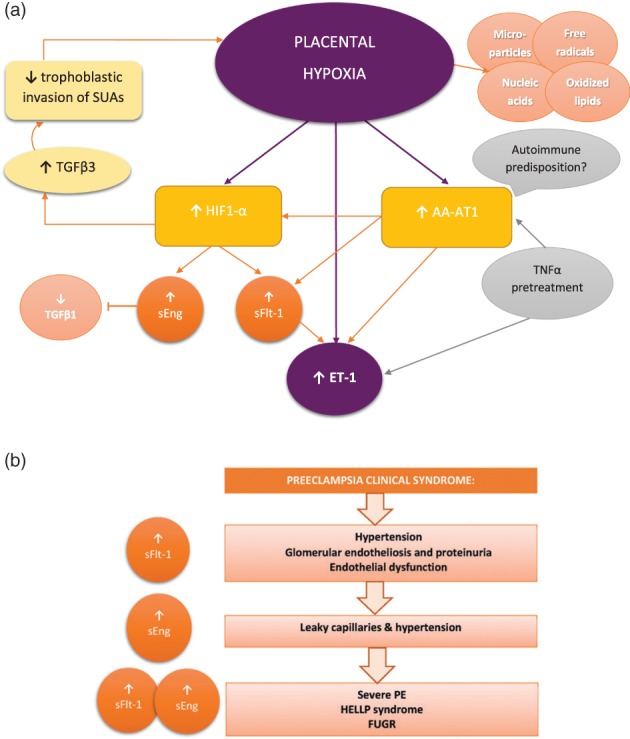
Pregnancy-related hypertension (PHTN) syndromes are a frequent and potentially deadly complication of pregnancy, while also negatively impacting the lifelong health of the mother and child. PHTN appears in women likely to develop hypertension later in life, with the stress of pregnancy unmasking a subclinical hypertensive phenotype. However, distinguishing between PHTN and chronic hypertension is essential for optimal management. Preeclampsia (PE) is linked to potentially severe outcomes and lacks effective treatments due to poorly understood mechanisms. Inadequate remodeling of spiral uterine arteries (SUAs), the cornerstone of PE pathophysiology, leads to hypoperfusion of the developing placenta. In normal pregnancies, extravillous trophoblast (EVT) cells assume an invasive phenotype and invade SUAs, transforming them into large conduits. Decidual natural killer cells play an essential role, mediating materno-fetal immune tolerance, inducing early SUA remodeling and regulating EVT invasiveness. Notch signaling is important in EVT phenotypic switch and is dysregulated in PE. The hypoxic placenta releases antiangiogenic and proinflammatory factors that converge upon maternal endothelium, inducing endothelial dysfunction, hypertension, and organ damage. Hypoxia-inducible factor 1-α is upstream of such molecules, whereas endothelin-1 is a major effector. We also describe important genetic links and evidence of incomplete materno-fetal immune tolerance, with PE patients presenting with autoantibodies, lower Treg , and higher Th 17 cells. Thus, PE manifestations arise as a consequence of mal-placentation or/and because of a predisposition of the maternal vascular bed to excessively react to pathogenic molecules. From this pathophysiological basis, we provide current and propose future therapeutic directions for PE.
Keywords: Decidual Natural Killer Cells; Extravillous Trophoblast Cells; Hypoxia; Incomplete Materno-Fetal Immune Tolerance; Preeclampsia.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
-
- Vest AR, Cho LS. Hypertension in pregnancy. Curr Atheroscler Rep. 2014;16:395. - PubMed
-
- American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in pregnancy . Report of the American College of Obstetricians and Gynecologists' Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122:1122–1131. - PubMed
-
- Breathett K, Muhlestein D, Foraker R, et al. Differences in preeclampsia rates between African American and Caucasian women: trends from the National Hospital Discharge Survey. J Womens Health (Larchmt). 2014;23:886–893. - PubMed
-
- Sibai B, Dekker G, Kupferminc M. Pre‐eclampsia. Lancet. 2005;365:785–799. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
