

Balanced Crystalloids versus Saline in Noncritically Ill Adults
- PMID: 29485926
- PMCID: PMC5846618
- DOI: 10.1056/NEJMoa1711586
Balanced Crystalloids versus Saline in Noncritically Ill Adults
Abstract
Background: Comparative clinical effects of balanced crystalloids and saline are uncertain, particularly in noncritically ill patients cared for outside an intensive care unit (ICU).
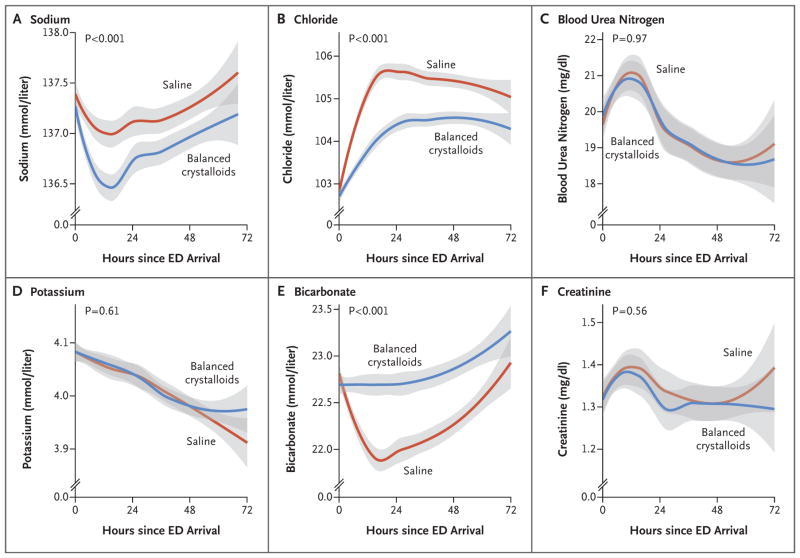
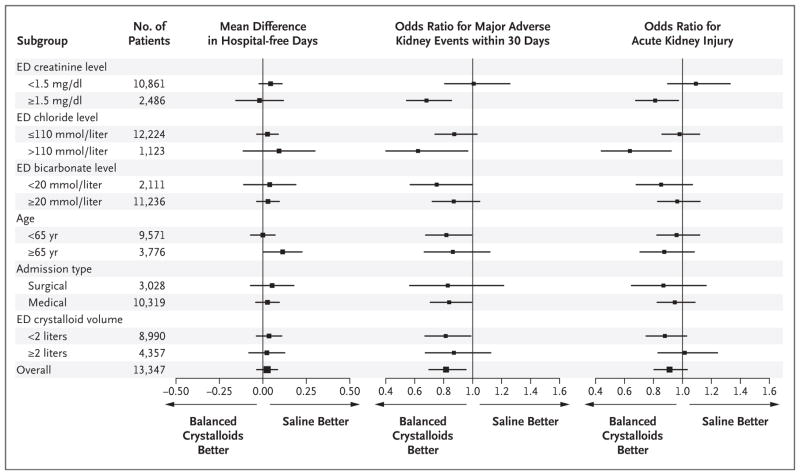
Methods: We conducted a single-center, pragmatic, multiple-crossover trial comparing balanced crystalloids (lactated Ringer's solution or Plasma-Lyte A) with saline among adults who were treated with intravenous crystalloids in the emergency department and were subsequently hospitalized outside an ICU. The type of crystalloid that was administered in the emergency department was assigned to each patient on the basis of calendar month, with the entire emergency department crossing over between balanced crystalloids and saline monthly during the 16-month trial. The primary outcome was hospital-free days (days alive after discharge before day 28). Secondary outcomes included major adverse kidney events within 30 days - a composite of death from any cause, new renal-replacement therapy, or persistent renal dysfunction (defined as an elevation of the creatinine level to ≥200% of baseline) - all censored at hospital discharge or 30 days, whichever occurred first.
Results: A total of 13,347 patients were enrolled, with a median crystalloid volume administered in the emergency department of 1079 ml and 88.3% of the patients exclusively receiving the assigned crystalloid. The number of hospital-free days did not differ between the balanced-crystalloids and saline groups (median, 25 days in each group; adjusted odds ratio with balanced crystalloids, 0.98; 95% confidence interval [CI], 0.92 to 1.04; P=0.41). Balanced crystalloids resulted in a lower incidence of major adverse kidney events within 30 days than saline (4.7% vs. 5.6%; adjusted odds ratio, 0.82; 95% CI, 0.70 to 0.95; P=0.01).
Conclusions: Among noncritically ill adults treated with intravenous fluids in the emergency department, there was no difference in hospital-free days between treatment with balanced crystalloids and treatment with saline. (Funded by the Vanderbilt Institute for Clinical and Translational Research and others; SALT-ED ClinicalTrials.gov number, NCT02614040 .).
Conflict of interest statement
Dr. Self reports receiving advisory board fees from Venaxis, Cempra Pharmaceuticals, Ferring Pharmaceuticals, and Biotest, consulting fees from Abbott Point of Care, and travel support from Gilead Sciences; and Dr. Rice, receiving consulting fees from Cumberland Pharmaceuticals and Avisa Pharma. No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Patient-Centered Outcomes and Resuscitation Fluids.N Engl J Med. 2018 Mar 1;378(9):862-863. doi: 10.1056/NEJMe1800449. Epub 2018 Feb 27. N Engl J Med. 2018. PMID: 29485927 No abstract available.
-
Isotonic fluids for volume resuscitation: is it really 6 liters of one, half a dozen of another?Kidney Int. 2018 Jun;93(6):1262-1264. doi: 10.1016/j.kint.2018.04.003. Kidney Int. 2018. PMID: 29792267 No abstract available.
-
Selection of Intravenous Fluids.Am J Kidney Dis. 2018 Dec;72(6):900-902. doi: 10.1053/j.ajkd.2018.05.007. Epub 2018 Jul 3. Am J Kidney Dis. 2018. PMID: 29980374 Free PMC article. No abstract available.
References
-
- Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med. 2013;369:1243–51. - PubMed
-
- Young P. Saline is the solution for crystalloid resuscitation. Crit Care Med. 2016;44:1538–40. - PubMed
-
- Bullivant EM, Wilcox CS, Welch WJ. Intrarenal vasoconstriction during hyperchloremia: role of thromboxane. Am J Physiol. 1989;256:F152–F157. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical