

The potential impact of case-area targeted interventions in response to cholera outbreaks: A modeling study
- PMID: 29485987
- PMCID: PMC5828347
- DOI: 10.1371/journal.pmed.1002509
The potential impact of case-area targeted interventions in response to cholera outbreaks: A modeling study
Abstract
Background: Cholera prevention and control interventions targeted to neighbors of cholera cases (case-area targeted interventions [CATIs]), including improved water, sanitation, and hygiene, oral cholera vaccine (OCV), and prophylactic antibiotics, may be able to efficiently avert cholera cases and deaths while saving scarce resources during epidemics. Efforts to quickly target interventions to neighbors of cases have been made in recent outbreaks, but little empirical evidence related to the effectiveness, efficiency, or ideal design of this approach exists. Here, we aim to provide practical guidance on how CATIs might be used by exploring key determinants of intervention impact, including the mix of interventions, "ring" size, and timing, in simulated cholera epidemics fit to data from an urban cholera epidemic in Africa.
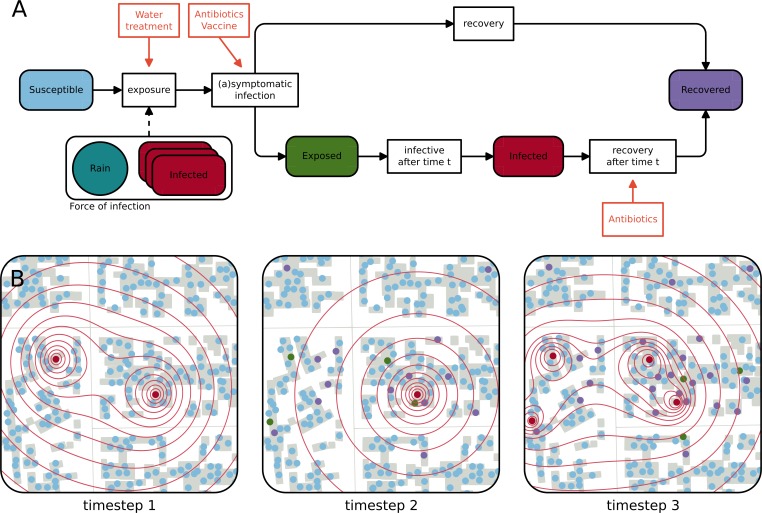
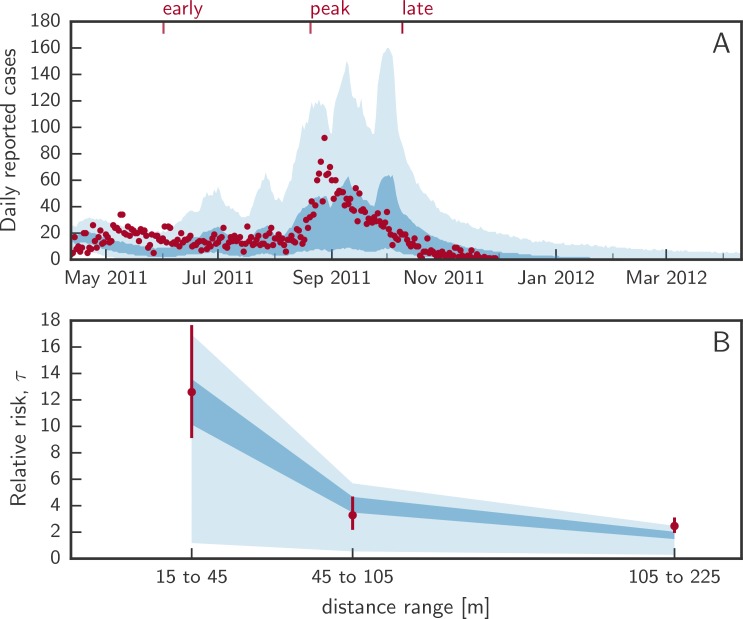
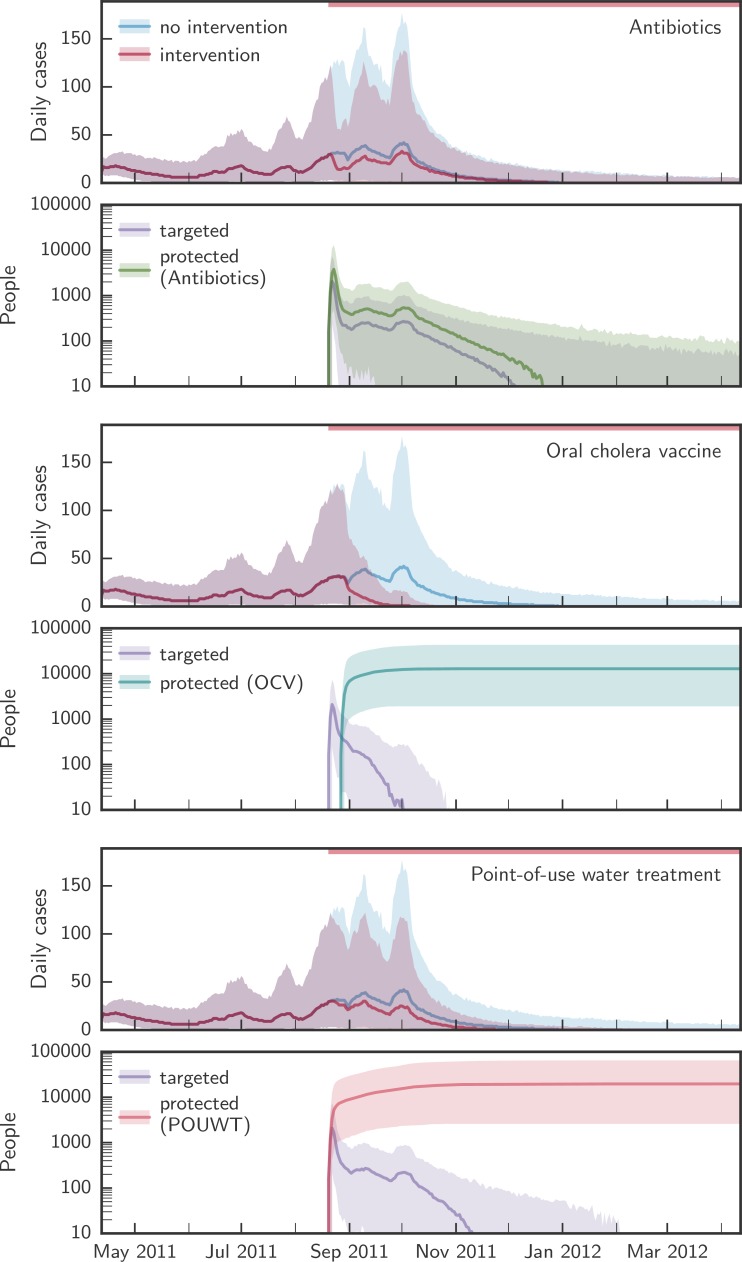
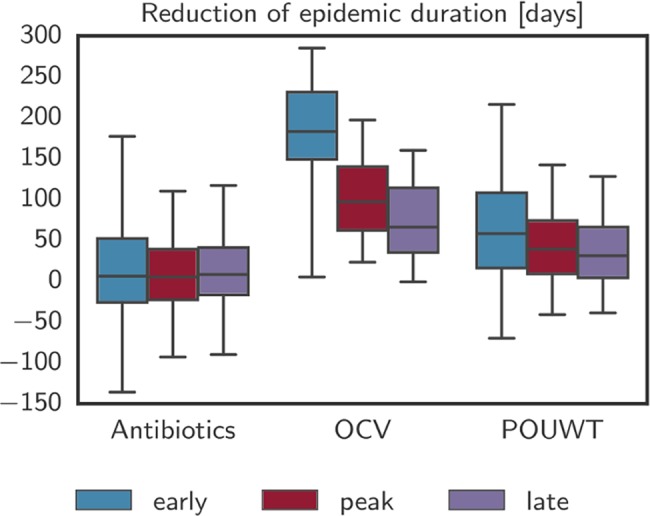
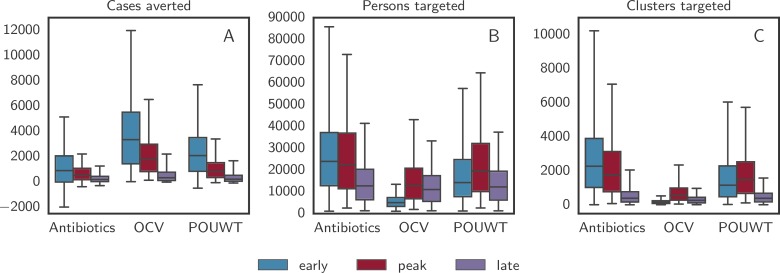
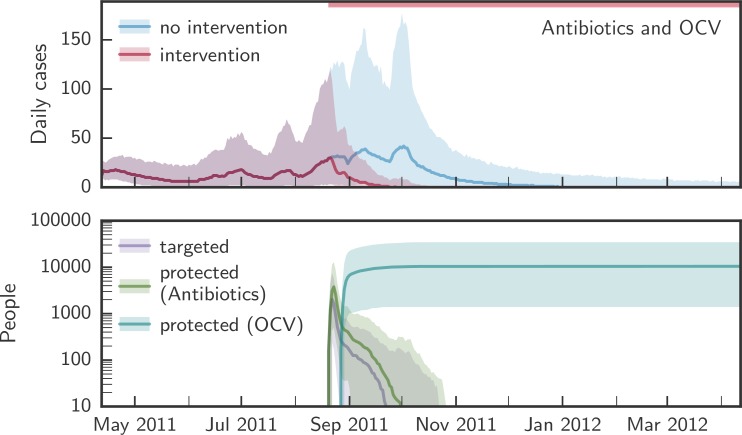
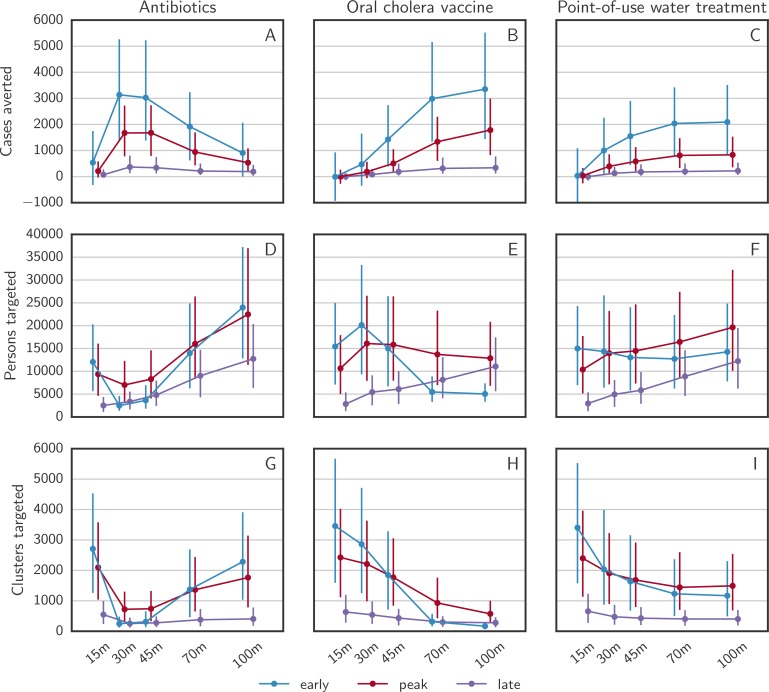
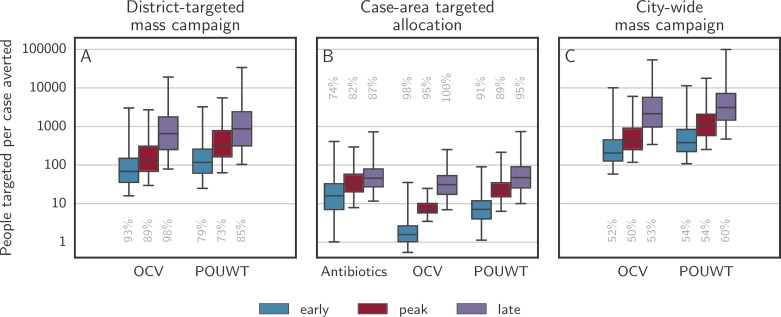
Methods and findings: We developed a micro-simulation model and calibrated it to both the epidemic curve and the small-scale spatiotemporal clustering pattern of case households from a large 2011 cholera outbreak in N'Djamena, Chad (4,352 reported cases over 232 days), and explored the potential impact of CATIs in simulated epidemics. CATIs were implemented with realistic logistical delays after cases presented for care using different combinations of prophylactic antibiotics, OCV, and/or point-of-use water treatment (POUWT) starting at different points during the epidemics and targeting rings of various radii around incident case households. Our findings suggest that CATIs shorten the duration of epidemics and are more resource-efficient than mass campaigns. OCV was predicted to be the most effective single intervention, followed by POUWT and antibiotics. CATIs with OCV started early in an epidemic focusing on a 100-m radius around case households were estimated to shorten epidemics by 68% (IQR 62% to 72%), with an 81% (IQR 69% to 87%) reduction in cases compared to uncontrolled epidemics. These same targeted interventions with OCV led to a 44-fold (IQR 27 to 78) reduction in the number of people needed to target to avert a single case of cholera, compared to mass campaigns in high-cholera-risk neighborhoods. The optimal radius to target around incident case households differed by intervention type, with antibiotics having an optimal radius of 30 m to 45 m compared to 70 m to 100 m for OCV and POUWT. Adding POUWT or antibiotics to OCV provided only marginal impact and efficiency improvements. Starting CATIs early in an epidemic with OCV and POUWT targeting those within 100 m of an incident case household reduced epidemic durations by 70% (IQR 65% to 75%) and the number of cases by 82% (IQR 71% to 88%) compared to uncontrolled epidemics. CATIs used late in epidemics, even after the peak, were estimated to avert relatively few cases but substantially reduced the number of epidemic days (e.g., by 28% [IQR 15% to 45%] for OCV in a 100-m radius). While this study is based on a rigorous, data-driven approach, the relatively high uncertainty about the ways in which POUWT and antibiotic interventions reduce cholera risk, as well as the heterogeneity in outbreak dynamics from place to place, limits the precision and generalizability of our quantitative estimates.
Conclusions: In this study, we found that CATIs using OCV, antibiotics, and water treatment interventions at an appropriate radius around cases could be an effective and efficient way to fight cholera epidemics. They can provide a complementary and efficient approach to mass intervention campaigns and may prove particularly useful during the initial phase of an outbreak, when there are few cases and few available resources, or in order to shorten the often protracted tails of cholera epidemics.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: JL is a paid statistical advisor for PLOS Medicine.
Figures
References
-
- World Health Organization. Cholera, 2016. Wkly Epidemiol Rec. 2017;92(36):521–36. - PubMed
-
- Ali M, Nelson AR, Lopez AL, Sack DA. Updated global burden of cholera in endemic countries. PLoS Negl Trop Dis. 2015;9(6):e0003832 doi: 10.1371/journal.pntd.0003832 - DOI - PMC - PubMed
-
- Luquero FJ, Rondy M, Boncy J, Munger A, Mekaoui H, Rymshaw E, et al. Mortality rates during cholera epidemic, Haiti, 2010–2011. Emerg Infect Dis. 2016;22(3):410–6. doi: 10.3201/eid2203.141970 - DOI - PMC - PubMed
-
- Rebaudet S, Sudre B, Faucher B, Piarroux R. Cholera in coastal Africa: a systematic review of its heterogeneous environmental determinants. J Infect Dis. 2013;208(Suppl 1):S98–106. doi: 10.1093/infdis/jit202 - DOI - PubMed
-
- Rebaudet S, Sudre B, Faucher B, Piarroux R. Environmental determinants of cholera outbreaks in inland Africa: a systematic review of main transmission foci and propagation routes. J Infect Dis. 2013;208(Suppl 1):S46–54. doi: 10.1093/infdis/jit195 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
