

Effectiveness of integrated care including therapeutic assertive community treatment in severe schizophrenia-spectrum and bipolar I disorders: Four-year follow-up of the ACCESS II study
- PMID: 29485988
- PMCID: PMC5828355
- DOI: 10.1371/journal.pone.0192929
Effectiveness of integrated care including therapeutic assertive community treatment in severe schizophrenia-spectrum and bipolar I disorders: Four-year follow-up of the ACCESS II study
Abstract
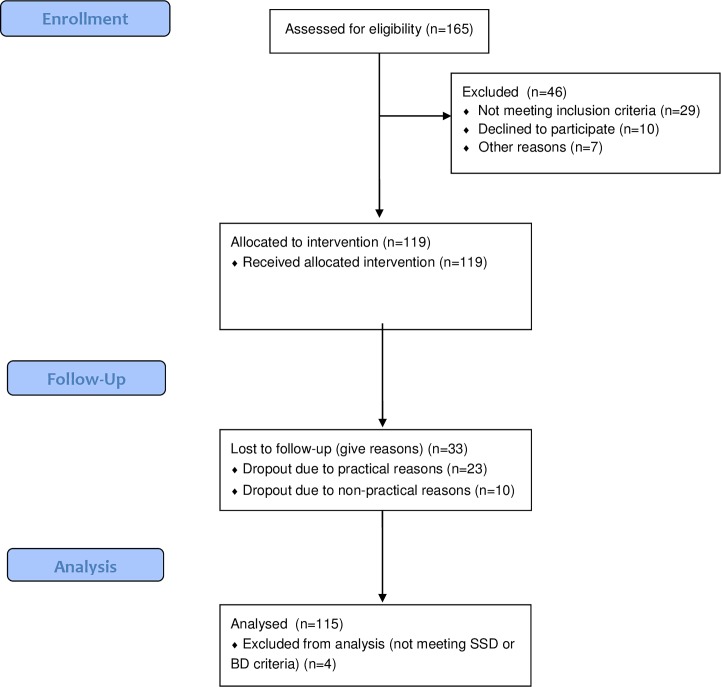
The ACCESS-model offers integrated care including assertive community treatment to patients with psychotic disorders. ACCESS proved more effective compared to standard care (ACCESS-I study) and was successfully implemented into clinical routine (ACCESS-II study). In this article, we report the 4-year outcomes of the ACCESS-II study. Between May 2007 and December 2013, 115 patients received continuous ACCESS-care. We hypothesized that the low 2-year disengagement and hospitalization rates and significant improvements in psychopathology, functioning, and quality of life could be sustained over 4 years. Over 4 years, only 10 patients disengaged from ACCESS. Another 23 left for practical reasons and were successfully transferred to other services. Hospitalization rates remained low (13.0% in year 3; 9.1% in year 4). Involuntary admissions decreased from 35% in the 2 years prior to ACCESS to 8% over 4 years in ACCESS. Outpatient contacts remained stably high at 2.0-2.4 per week. We detected significant improvements in psychopathology (effect size d = 0.79), illness severity (d = 1.29), level of functioning (d = 0.77), quality of life (d = 0.47) and stably high client satisfaction (d = 0.02) over 4 years. Most positive effects were observed within the first 2 years with the exception of illness severity, which further improved from year 2 to 4. Within continuous intensive 4-year ACCESS-care, sustained improvements in psychopathology, functioning, quality of life, low service disengagement and re-hospitalization rates, as well as low rates of involuntary treatment, were observed in contrast to other studies, which reported a decline in these parameters once a specific treatment model was stopped. Yet, stronger evidence to prove these results is required.
Trial registration: Clinical Trial Registration Number: NCT01888627.
Conflict of interest statement
Figures
References
-
- NICE. Psychosis and Schizophrenia in Adults: NICE Guideline. In: Excellence NIfHaC, editor. London, UK: 2014.
-
- Austin SF, Mors O, Secher RG, Hjorthoj CR, Albert N, Bertelsen M, et al. Predictors of recovery in first episode psychosis: the OPUS cohort at 10 year follow-up. Schizophr Res. 2013;150(1):163–8. doi: 10.1016/j.schres.2013.07.031 . - DOI - PubMed
-
- Hafner H, Maurer K, An der Heiden W. [Schizophrenia—a disorder in its own right?: results from 25 years of the ABC study]. Nervenarzt. 2013;84(9):1093–4, 6–103. doi: 10.1007/s00115-013-3788-6 . - DOI - PubMed
-
- Lambert M, Bock T, Schottle D, Golks D, Meister K, Rietschel L, et al. Assertive community treatment as part of integrated care versus standard care: a 12-month trial in patients with first- and multiple-episode schizophrenia spectrum disorders treated with quetiapine immediate release (ACCESS trial). J Clin Psychiatry. 2010;71(10):1313–23. doi: 10.4088/JCP.09m05113yel . - DOI - PubMed
-
- Marshall M, Lockwood A. Assertive community treatment for people with severe mental disorders. Cochrane Database Syst Rev. 2000;(2):CD001089 doi: 10.1002/14651858.CD001089 . - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
