

Effect of Bag-Mask Ventilation vs Endotracheal Intubation During Cardiopulmonary Resuscitation on Neurological Outcome After Out-of-Hospital Cardiorespiratory Arrest: A Randomized Clinical Trial
- PMID: 29486039
- PMCID: PMC5838565
- DOI: 10.1001/jama.2018.0156
Effect of Bag-Mask Ventilation vs Endotracheal Intubation During Cardiopulmonary Resuscitation on Neurological Outcome After Out-of-Hospital Cardiorespiratory Arrest: A Randomized Clinical Trial
Abstract
Importance: Bag-mask ventilation (BMV) is a less complex technique than endotracheal intubation (ETI) for airway management during the advanced cardiac life support phase of cardiopulmonary resuscitation of patients with out-of-hospital cardiorespiratory arrest. It has been reported as superior in terms of survival.
Objectives: To assess noninferiority of BMV vs ETI for advanced airway management with regard to survival with favorable neurological function at day 28.
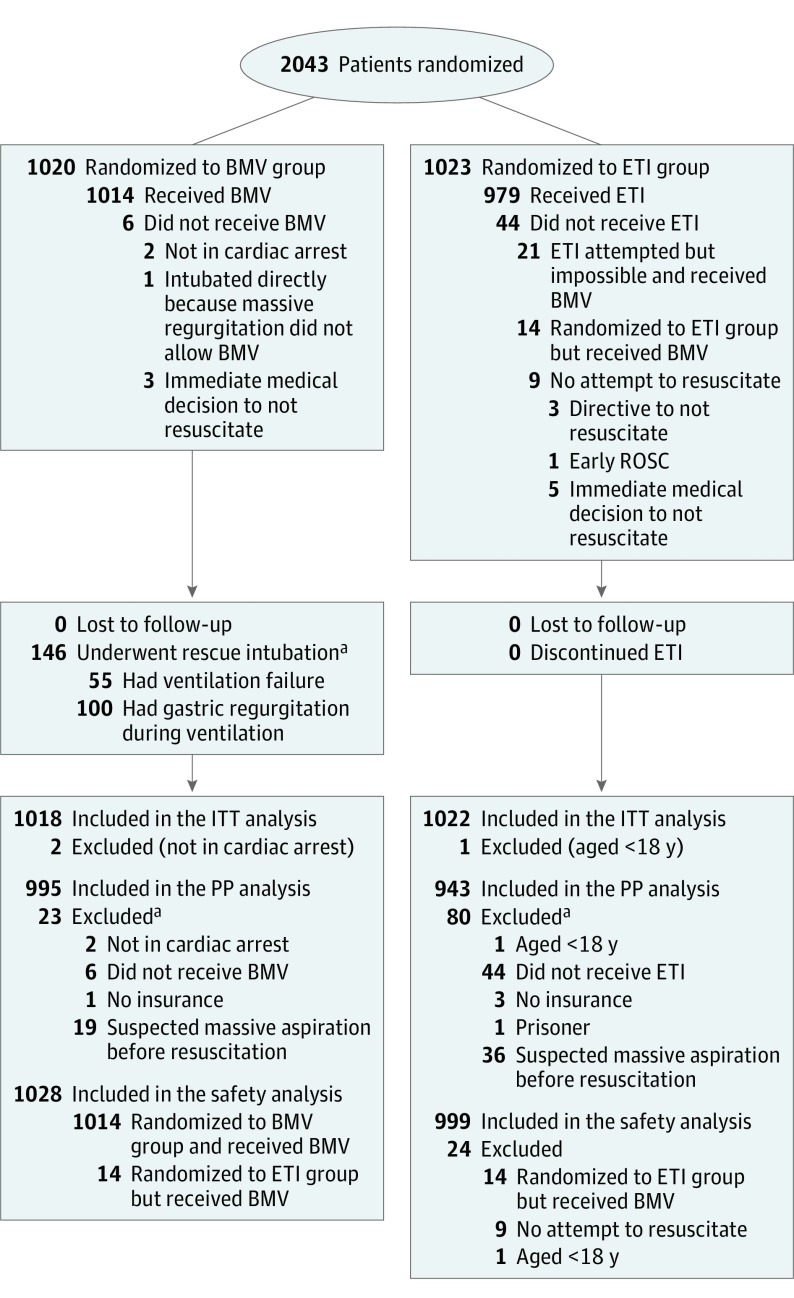
Design, settings, and participants: Multicenter randomized clinical trial comparing BMV with ETI in 2043 patients with out-of-hospital cardiorespiratory arrest in France and Belgium. Enrollment occurred from March 9, 2015, to January 2, 2017, and follow-up ended January 26, 2017.
Intervention: Participants were randomized to initial airway management with BMV (n = 1020) or ETI (n = 1023).
Main outcomes and measures: The primary outcome was favorable neurological outcome at 28 days defined as cerebral performance category 1 or 2. A noninferiority margin of 1% was chosen. Secondary end points included rate of survival to hospital admission, rate of survival at day 28, rate of return of spontaneous circulation, and ETI and BMV difficulty or failure.
Results: Among 2043 patients who were randomized (mean age, 64.7 years; 665 women [32%]), 2040 (99.8%) completed the trial. In the intention-to-treat population, favorable functional survival at day 28 was 44 of 1018 patients (4.3%) in the BMV group and 43 of 1022 patients (4.2%) in the ETI group (difference, 0.11% [1-sided 97.5% CI, -1.64% to infinity]; P for noninferiority = .11). Survival to hospital admission (294/1018 [28.9%] in the BMV group vs 333/1022 [32.6%] in the ETI group; difference, -3.7% [95% CI, -7.7% to 0.3%]) and global survival at day 28 (55/1018 [5.4%] in the BMV group vs 54/1022 [5.3%] in the ETI group; difference, 0.1% [95% CI, -1.8% to 2.1%]) were not significantly different. Complications included difficult airway management (186/1027 [18.1%] in the BMV group vs 134/996 [13.4%] in the ETI group; difference, 4.7% [95% CI, 1.5% to 7.9%]; P = .004), failure (69/1028 [6.7%] in the BMV group vs 21/996 [2.1%] in the ETI group; difference, 4.6% [95% CI, 2.8% to 6.4%]; P < .001), and regurgitation of gastric content (156/1027 [15.2%] in the BMV group vs 75/999 [7.5%] in the ETI group; difference, 7.7% [95% CI, 4.9% to 10.4%]; P < .001).
Conclusions and relevance: Among patients with out-of-hospital cardiorespiratory arrest, the use of BMV compared with ETI failed to demonstrate noninferiority or inferiority for survival with favorable 28-day neurological function, an inconclusive result. A determination of equivalence or superiority between these techniques requires further research.
Trial registration: clinicaltrials.gov Identifier: NCT02327026.
Conflict of interest statement
Figures
Comment in
-
Airway Management During Out-of-Hospital Cardiac Arrest.JAMA. 2018 Feb 27;319(8):771-772. doi: 10.1001/jama.2018.0155. JAMA. 2018. PMID: 29486014 No abstract available.
References
-
- Stiell IG, Wells GA, Field B, et al. ; Ontario Prehospital Advanced Life Support Study Group . Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351(7):647-656. - PubMed
-
- Wang C-H, Chen W-J, Chang W-T, et al. . The association between timing of tracheal intubation and outcomes of adult in-hospital cardiac arrest: a retrospective cohort study. Resuscitation. 2016;105:59-65. - PubMed
-
- McMullan J, Gerecht R, Bonomo J, et al. ; CARES Surveillance Group . Airway management and out-of-hospital cardiac arrest outcome in the CARES registry. Resuscitation. 2014;85(5):617-622. - PubMed
-
- Fouche PF, Simpson PM, Bendall J, Thomas RE, Cone DC, Doi SAR. Airways in out-of-hospital cardiac arrest: systematic review and meta-analysis. Prehosp Emerg Care. 2014;18(2):244-256. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
