

Effect of On-Demand vs Routine Nebulization of Acetylcysteine With Salbutamol on Ventilator-Free Days in Intensive Care Unit Patients Receiving Invasive Ventilation: A Randomized Clinical Trial
- PMID: 29486489
- PMCID: PMC5885882
- DOI: 10.1001/jama.2018.0949
Effect of On-Demand vs Routine Nebulization of Acetylcysteine With Salbutamol on Ventilator-Free Days in Intensive Care Unit Patients Receiving Invasive Ventilation: A Randomized Clinical Trial
Abstract
Importance: It remains uncertain whether nebulization of mucolytics with bronchodilators should be applied for clinical indication or preventively in intensive care unit (ICU) patients receiving invasive ventilation.
Objective: To determine if a strategy that uses nebulization for clinical indication (on-demand) is noninferior to one that uses preventive (routine) nebulization.
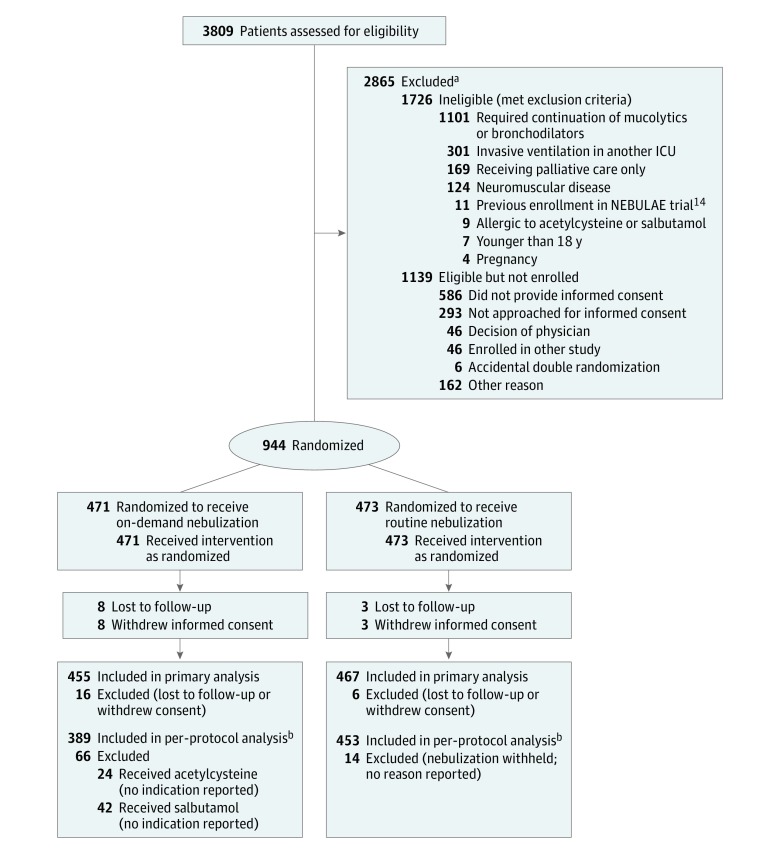
Design, setting, and participants: Randomized clinical trial enrolling adult patients expected to need invasive ventilation for more than 24 hours at 7 ICUs in the Netherlands.
Interventions: On-demand nebulization of acetylcysteine or salbutamol (based on strict clinical indications, n = 471) or routine nebulization of acetylcysteine with salbutamol (every 6 hours until end of invasive ventilation, n = 473).
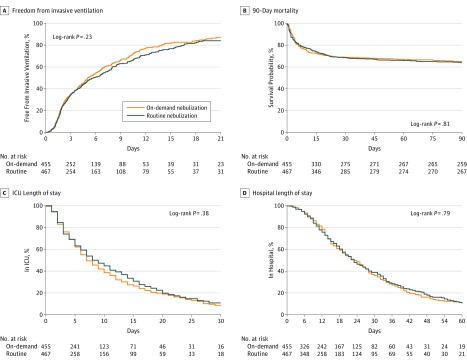
Main outcomes and measures: The primary outcome was the number of ventilator-free days at day 28, with a noninferiority margin for a difference between groups of -0.5 days. Secondary outcomes included length of stay, mortality rates, occurrence of pulmonary complications, and adverse events.
Results: Nine hundred twenty-two patients (34% women; median age, 66 (interquartile range [IQR], 54-75 years) were enrolled and completed follow-up. At 28 days, patients in the on-demand group had a median 21 (IQR, 0-26) ventilator-free days, and patients in the routine group had a median 20 (IQR, 0-26) ventilator-free days (1-sided 95% CI, -0.00003 to ∞). There was no significant difference in length of stay or mortality, or in the proportion of patients developing pulmonary complications, between the 2 groups. Adverse events (13.8% vs 29.3%; difference, -15.5% [95% CI, -20.7% to -10.3%]; P < .001) were more frequent with routine nebulization and mainly related to tachyarrhythmia (12.5% vs 25.9%; difference, -13.4% [95% CI, -18.4% to -8.4%]; P < .001) and agitation (0.2% vs 4.3%; difference, -4.1% [95% CI, -5.9% to -2.2%]; P < .001).
Conclusions and relevance: Among ICU patients receiving invasive ventilation who were expected to not be extubated within 24 hours, on-demand compared with routine nebulization of acetylcysteine with salbutamol did not result in an inferior number of ventilator-free days. On-demand nebulization may be a reasonable alternative to routine nebulization.
Trial registration: clinicaltrials.gov Identifier: NCT02159196.
Conflict of interest statement
Figures
Comment in
-
Precision medicine and aerosolization in mechanically ventilated adults.J Thorac Dis. 2018 Sep;10(Suppl 26):S3111-S3114. doi: 10.21037/jtd.2018.07.64. J Thorac Dis. 2018. PMID: 30370091 Free PMC article. No abstract available.
References
-
- Icard BL, Rubio E. The role of mucoactive agents in the mechanically ventilated patient: a review of the literature. Expert Rev Respir Med. 2017;11(10):807-814. - PubMed
-
- Konrad F, Schreiber T, Brecht-Kraus D, et al. Mucociliary transport in ICU patients. Chest. 1994;105:237-241. - PubMed
-
- Rubin BK. The pharmacologic approach to airway clearance: mucoactive agents. Respir Care. 2002;47(7):818-822. - PubMed
-
- Konrad F, Schoenberg MH, Wiedmann H, et al. The application of N-acetylcysteine as an antioxidant and mucolytic in mechanical ventilation in intensive care patients: a prospective, randomized, placebo-controlled, double-blind study. Anaesthesist. 1995;44(9):651-658. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
