

Case Reports
doi: 10.1002/hep.29858.
Epub 2018 Apr 27.
Glycogen storage disease type Ia: Adult presentation with microcytic anemia and liver adenomas
Affiliations
- PMID: 29486517
- PMCID: PMC6099216
- DOI: 10.1002/hep.29858
Item in Clipboard
Case Reports
Glycogen storage disease type Ia: Adult presentation with microcytic anemia and liver adenomas
Hepatology.
2018 Aug.
No abstract available
Figures
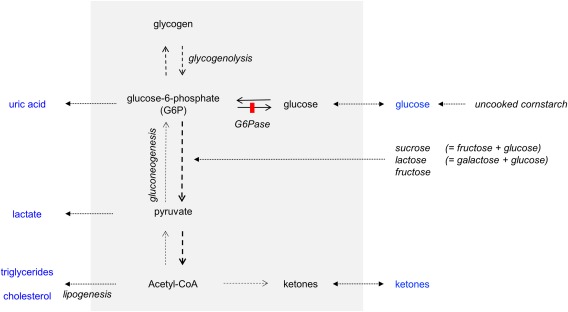
The effect of liver (gray) G6Pase deficiency on major pathways of endogenous glucose production (glycogenolysis and gluconeogenesis), ketogenesis, and lipogenesis during fasting. This simplified scheme explains the biochemical phenotype of hypo‐ or nonketotic hypoglycemia, hyperlactatecemia, hyperuricemia, and hyperlipidemia. Hepatomegaly is caused by storage of both glycogen and lipids. To compensate deficient endogenous glucose production, avoidance of fasting and regular meals are prescribed. Uncooked cornstarch is digested slowly and provides a steady release of exogenous glucose molecules, compared to simple sugars. To prevent nocturnal hypoglycemias, either cornstarch‐enriched feedings every 3‐4 hours (especially for infants, some adult GSD Ia patients may eventually need only one bedtime dose) are offered, or alternatively continuous gastric drip feeding. Because dietary fructose and galactose cannot be metabolized from G6P toward glucose, they contribute to the metabolic perturbation. Therefore, these dietary sugars are often restricted or avoided. Abbreviation: Acetyl‐CoA, acetyl coenzyme A.
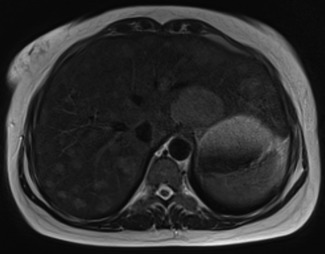
Abdominal MRI image from our patient displaying hepatomegaly and multiple hepatocellular adenomas. On the T2‐weighted image, many mildly hyperintense lesions are visible diffusely distributed in all liver segments, with a maximum diameter of 4.6 cm. The lesions showed arterial enhancement after administration of intravenous contrast material, persisting in the portal venous phase, consistent with hepatocellular adenomas (not shown). During the second trimester of her pregnancy, follow‐up MRI in August 2017 displayed no significant changes compared to the initial MRI. After an uneventful pregnancy and Caesarian section in November 2017, follow‐up MRI in February 2018 showed significant decrease in adenoma size, with the largest lesion measuring 4.1 cm (not shown). Based on the initial MRI and CT images of our patient, an interactive 3D model was created presenting the hepatomegaly, hepatocellular adenomas (in blue), and renomegaly in our patient (https://skfb.ly/6uEvD ). Abbreviation: 3D, three‐dimensional; CT, computed tomography; MRI, magnetic resonance imaging.
Similar articles
-
[Multiple large hepatocellular adenomas in a patient with glycogen storage disease type Ia].Nihon Shokakibyo Gakkai Zasshi. 2014 Apr;111(4):787-96. Nihon Shokakibyo Gakkai Zasshi. 2014. PMID: 24769469 Japanese.
-
Fifteen years of follow-up of a liver transplant recipient with glycogen storage disease type Ia (Von Gierke disease).Transplant Proc. 2013;45(10):3668-9. doi: 10.1016/j.transproceed.2013.10.033. Transplant Proc. 2013. PMID: 24314991
-
Magnetic resonance imaging findings of hepatic adenomas in von Gierke (type I) glycogen storage disease: case report.Can Assoc Radiol J. 1999 Jun;50(3):161-4. Can Assoc Radiol J. 1999. PMID: 10405647 No abstract available.
-
Prevention of complications in glycogen storage disease type Ia with optimization of metabolic control.Pediatr Diabetes. 2017 Aug;18(5):327-331. doi: 10.1111/pedi.12540. Epub 2017 Jun 1. Pediatr Diabetes. 2017. PMID: 28568353 Review.
-
Hepatocellular adenomas in glycogen storage disease type I and III: a series of 43 patients and review of the literature.J Pediatr Gastroenterol Nutr. 1997 Mar;24(3):276-9. doi: 10.1097/00005176-199703000-00008. J Pediatr Gastroenterol Nutr. 1997. PMID: 9138172 Review.
Cited by
-
Dynamic Methods for Childhood Hypoglycemia Phenotyping: A Narrative Review.Front Endocrinol (Lausanne). 2022 Jun 17;13:858832. doi: 10.3389/fendo.2022.858832. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35789807 Free PMC article. Review.
-
A case study of glycogen storage disease type Ia presenting with multiple hepatocellular adenomas: an analysis by gadolinium ethoxybenzyl-diethylenetriamine-pentaacetic acid magnetic resonance imaging.Quant Imaging Med Surg. 2021 Jun;11(6):2785-2791. doi: 10.21037/qims-20-746. Quant Imaging Med Surg. 2021. PMID: 34079743 Free PMC article.
-
Glycogen Storage Disease Type Ia: Current Management Options, Burden and Unmet Needs.Nutrients. 2021 Oct 27;13(11):3828. doi: 10.3390/nu13113828. Nutrients. 2021. PMID: 34836082 Free PMC article. Review.
-
A case report of acute pancreatitis with glycogen storage disease type IA in an adult patient and review of the literature.Medicine (Baltimore). 2020 Oct 16;99(42):e22644. doi: 10.1097/MD.0000000000022644. Medicine (Baltimore). 2020. PMID: 33080702 Free PMC article. Review.
-
High childhood serum triglyceride concentrations associate with hepatocellular adenoma development in patients with glycogen storage disease type Ia.JHEP Rep. 2022 May 29;4(8):100512. doi: 10.1016/j.jhepr.2022.100512. eCollection 2022 Aug. JHEP Rep. 2022. PMID: 35811762 Free PMC article.
References
-
- Bali DS, Chen YT, Austin S, Goldstein JL. Glycogen Storage Disease Type I. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJ, et al, eds. Seattle, WA: GeneReviews(R); 1993. - PubMed
-
- Cassiman D, Libbrecht L, Verslype C, Meersseman W, Troisi R, Zucman‐Rossi J, et al. An adult male patient with multiple adenomas and a hepatocellular carcinoma: mild glycogen storage disease type Ia. J Hepatol 2010;53:213‐217. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
