

Splash M-knife versus Flush Knife BT in the technical outcomes of endoscopic submucosal dissection for early gastric cancer: a propensity score matching analysis
- PMID: 29486717
- PMCID: PMC5832194
- DOI: 10.1186/s12876-018-0763-5
Splash M-knife versus Flush Knife BT in the technical outcomes of endoscopic submucosal dissection for early gastric cancer: a propensity score matching analysis
Abstract
Background: Endoscopic submucosal dissection (ESD) is a standard treatment for early gastric cancer. A new multi-functional ESD device was developed to achieve complete ESD with a single device. A metal plate attached to its distal sheath achieves better hemostasis during the procedure than the other needle-knife device, Flush Knife BT®, that has been conventionally used. The aim of this study was to compare the technical outcomes of ESD for early gastric cancer using the Splash M-Knife® with those using the Flush Knife BT.
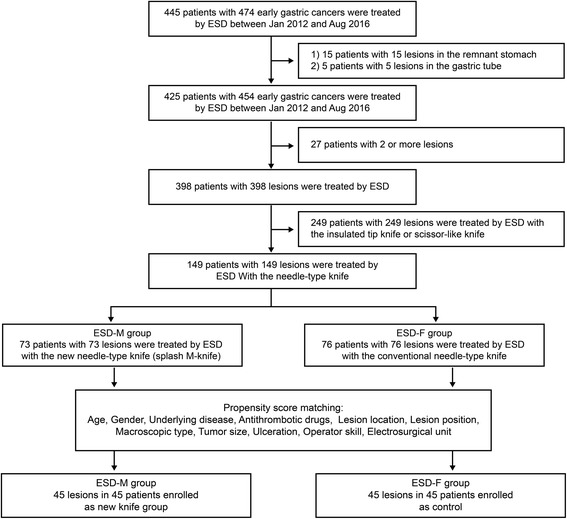
Methods: We conducted a retrospective review of the case records of 149 patients with early gastric cancer treated with ESD using the needle-type ESD knives between January 2012 and August 2016 at Kitakyushu Municipal Medical Center. Lesions treated with ESD using the Splash M-knife (ESD-M) and the Flush Knife BT (ESD-F) were compared. Multivariate analyses and propensity score matching were used to compensate for the differences in age, gender, underlying disease, antithrombotic drug use, lesion location, lesion position, macroscopic type, tumor size, presence of ulceration, operator level and types of electrosurgical unit used. The primary endpoint was the requirement to use hemostatic forceps in the two groups. The secondary endpoints of procedure time, en bloc and complete resection rates, and adverse events rates were evaluated for the two groups.
Results: There were 73 patients in the ESD-M group, and 76 patients in the ESD-F group. Propensity score matching analysis created 45 matched pairs. Adjusted comparisons between the two groups showed a significantly lower usage rate of hemostatic forceps in the ESD-M group than in the ESD-F group (6.7% vs 84.4%, p < 0.001). Treatment outcomes showed an en bloc resection rate of 100% in both groups; complete resection rate of 95.6% vs 100%, p = 0.49; median procedure time of 74.0 min vs 71.0 min, p = 0.90; post-procedure bleeding of 2.2% vs 2.2%, p = 1, in the ESD-M and ESD-F groups, respectively. There were no perforations in either group.
Conclusions: ESD-M appeared to reduce the usage of hemostatic forceps during ESD for early gastric cancer without increasing the adverse effects. Thus, it may contribute to a reduction in the total ESD cost.
Keywords: Device; Early gastric cancer; Endoscopic submucosal dissection; Hemostasis; Splash M-knife.
Conflict of interest statement
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. This study protocol was approved by the institutional review board of Kitakyushu Municipal Medical Center on November 18, 2016. Written informed consent was obtained from all patients before ESD.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
