

Vasoplegia treatments: the past, the present, and the future
- PMID: 29486781
- PMCID: PMC6389278
- DOI: 10.1186/s13054-018-1967-3
Vasoplegia treatments: the past, the present, and the future
Abstract
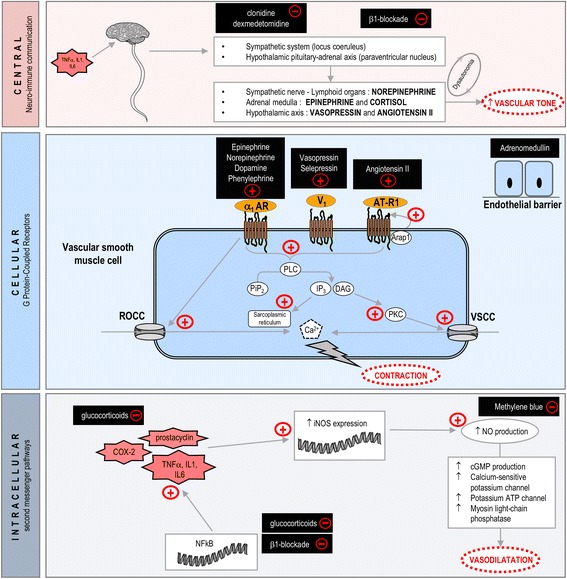
Vasoplegia is a ubiquitous phenomenon in all advanced shock states, including septic, cardiogenic, hemorrhagic, and anaphylactic shock. Its pathophysiology is complex, involving various mechanisms in vascular smooth muscle cells such as G protein-coupled receptor desensitization (adrenoceptors, vasopressin 1 receptors, angiotensin type 1 receptors), alteration of second messenger pathways, critical illness-related corticosteroid insufficiency, and increased production of nitric oxide. This review, based on a critical appraisal of the literature, discusses the main current treatments and future approaches. Our improved understanding of these mechanisms is progressively changing our therapeutic approach to vasoplegia from a standardized to a personalized multimodal treatment with the prescription of several vasopressors. While norepinephrine is confirmed as first line therapy for the treatment of vasoplegia, the latest Surviving Sepsis Campaign guidelines also consider that the best therapeutic management of vascular hyporesponsiveness to vasopressors could be a combination of multiple vasopressors, including norepinephrine and early prescription of vasopressin. This new approach is seemingly justified by the need to limit adrenoceptor desensitization as well as sympathetic overactivation given its subsequent deleterious impacts on hemodynamics and inflammation. Finally, based on new pathophysiological data, two potential drugs, selepressin and angiotensin II, are currently being evaluated.
Keywords: Catecholamines; Circulatory failure; Septic shock; Vasoconstrictor agents; Vasoplegic syndrome.
Conflict of interest statement
Author information
Not applicable.
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors read and approved the final manuscript.
Competing interests
The authors have disclosed that they do not have any potential conflicts of interest related to this work.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
The mechanism of action of the adrenomedullin-binding antibody adrecizumab.Crit Care. 2018 Jun 13;22(1):159. doi: 10.1186/s13054-018-2074-1. Crit Care. 2018. PMID: 29895302 Free PMC article. No abstract available.
References
-
- Kimmoun A, Ducrocq N, Levy B. Mechanisms of vascular hyporesponsiveness in septic shock. Curr Vasc Pharmacol. 2013;11:139–149. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
